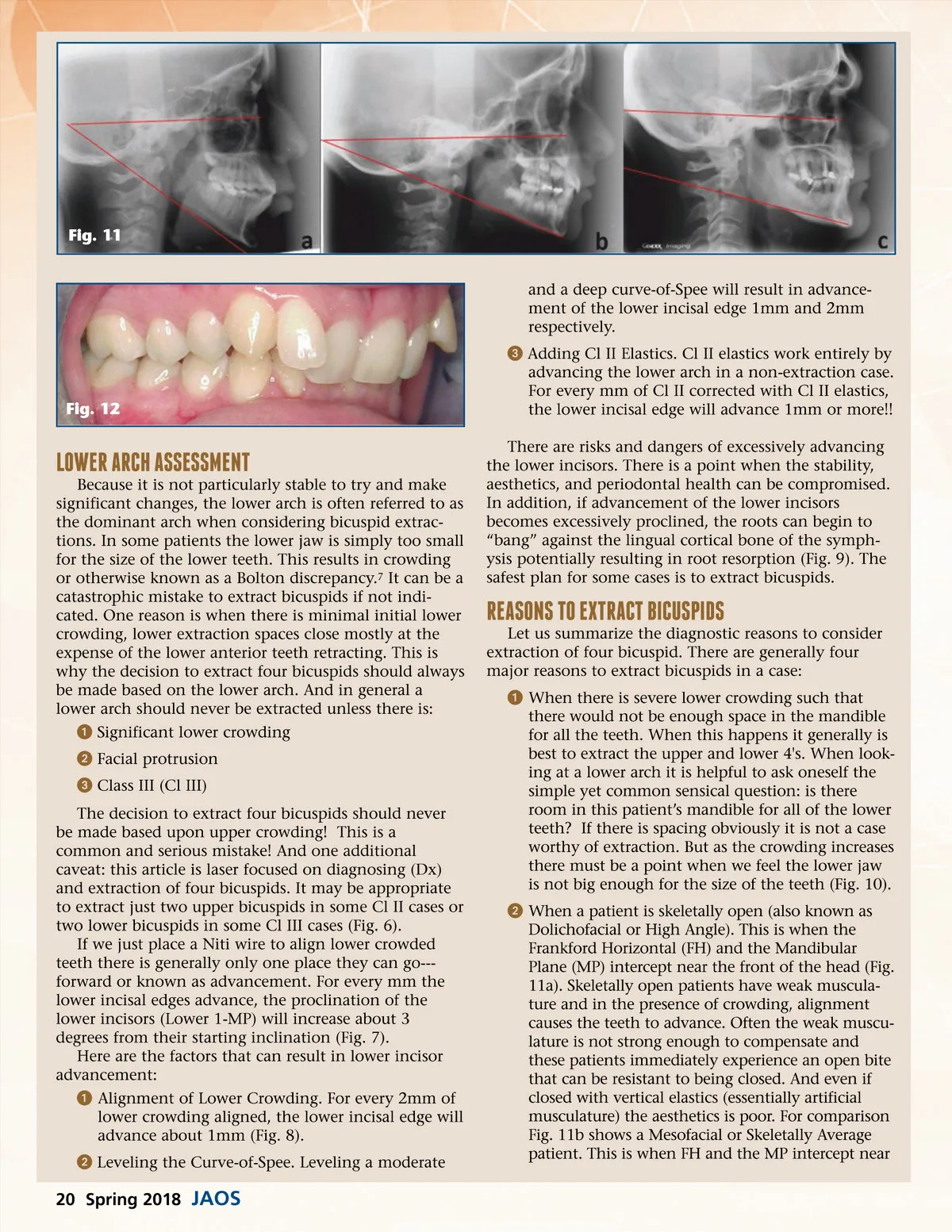
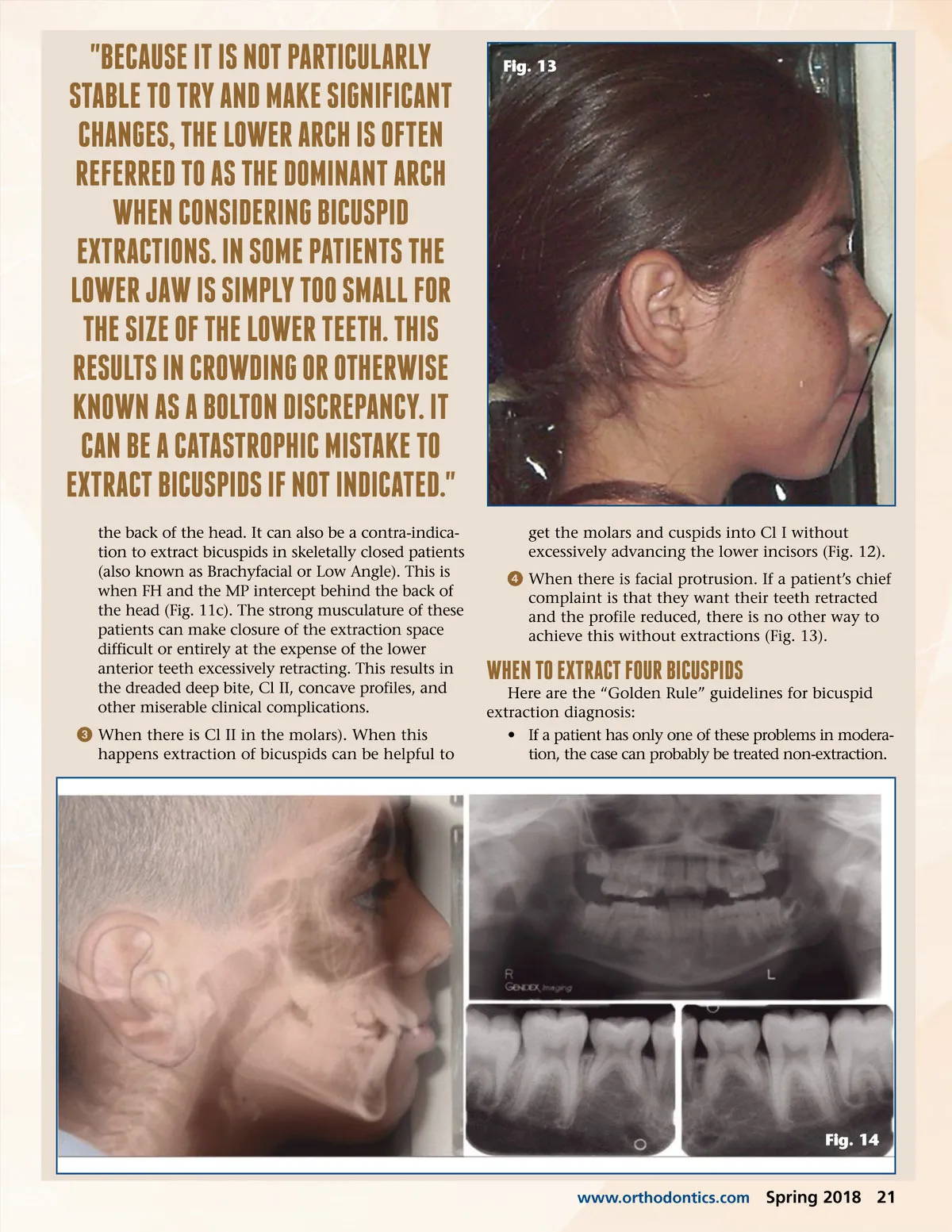
Fig. 11 and a deep curve-of-Spee will result in advance-ment of the lower incisal edge 1mm and 2mm respectively. ᕣ Adding Cl II Elastics. Cl II elastics work entirely by advancing the lower arch in a non-extraction case. For every mm of Cl II corrected with Cl II elastics, the lower incisal edge will advance 1mm or more!! There are risks and dangers of excessively advancing the lower incisors. There is a point when the stability, aesthetics, and periodontal health can be compromised. In addition, if advancement of the lower incisors becomes excessively proclined, the roots can begin to “bang” against the lingual cortical bone of the symph-ysis potentially resulting in root resorption (Fig. 9). The safest plan for some cases is to extract bicuspids. Fig. 12 lowER ARCh ASSESSMEnT Because it is not particularly stable to try and make significant changes, the lower arch is often referred to as the dominant arch when considering bicuspid extrac-tions. In some patients the lower jaw is simply too small for the size of the lower teeth. This results in crowding or otherwise known as a Bolton discrepancy. 7 It can be a catastrophic mistake to extract bicuspids if not indi-cated. One reason is when there is minimal initial lower crowding, lower extraction spaces close mostly at the expense of the lower anterior teeth retracting. This is why the decision to extract four bicuspids should always be made based on the lower arch. And in general a lower arch should never be extracted unless there is: ᕡ Significant lower crowding ᕢ Facial protrusion ᕣ Class III (Cl III) The decision to extract four bicuspids should never be made based upon upper crowding! This is a common and serious mistake! And one additional caveat: this article is laser focused on diagnosing (Dx) and extraction of four bicuspids. It may be appropriate to extract just two upper bicuspids in some Cl II cases or two lower bicuspids in some Cl III cases (Fig. 6). If we just place a Niti wire to align lower crowded teeth there is generally only one place they can go---forward or known as advancement. For every mm the lower incisal edges advance, the proclination of the lower incisors (Lower 1-MP) will increase about 3 degrees from their starting inclination (Fig. 7). Here are the factors that can result in lower incisor advancement: ᕡ Alignment of Lower Crowding. For every 2mm of lower crowding aligned, the lower incisal edge will advance about 1mm (Fig. 8). ᕢ Leveling the Curve-of-Spee. Leveling a moderate REASonS To EXTRACT BiCuSPiDS Let us summarize the diagnostic reasons to consider extraction of four bicuspid. There are generally four major reasons to extract bicuspids in a case: ᕡ When there is severe lower crowding such that there would not be enough space in the mandible for all the teeth. When this happens it generally is best to extract the upper and lower 4's. When look-ing at a lower arch it is helpful to ask oneself the simple yet common sensical question: is there room in this patient’s mandible for all of the lower teeth? If there is spacing obviously it is not a case worthy of extraction. But as the crowding increases there must be a point when we feel the lower jaw is not big enough for the size of the teeth (Fig. 10). ᕢ When a patient is skeletally open (also known as Dolichofacial or High Angle). This is when the Frankford Horizontal (FH) and the Mandibular Plane (MP) intercept near the front of the head (Fig. 11a). Skeletally open patients have weak muscula-ture and in the presence of crowding, alignment causes the teeth to advance. Often the weak muscu-lature is not strong enough to compensate and these patients immediately experience an open bite that can be resistant to being closed. And even if closed with vertical elastics (essentially artificial musculature) the aesthetics is poor. For comparison Fig. 11b shows a Mesofacial or Skeletally Average patient. This is when FH and the MP intercept near 20 Spring 2018 JAOS
Journal of the American Orthodontic Society Spring 2018: Page 20