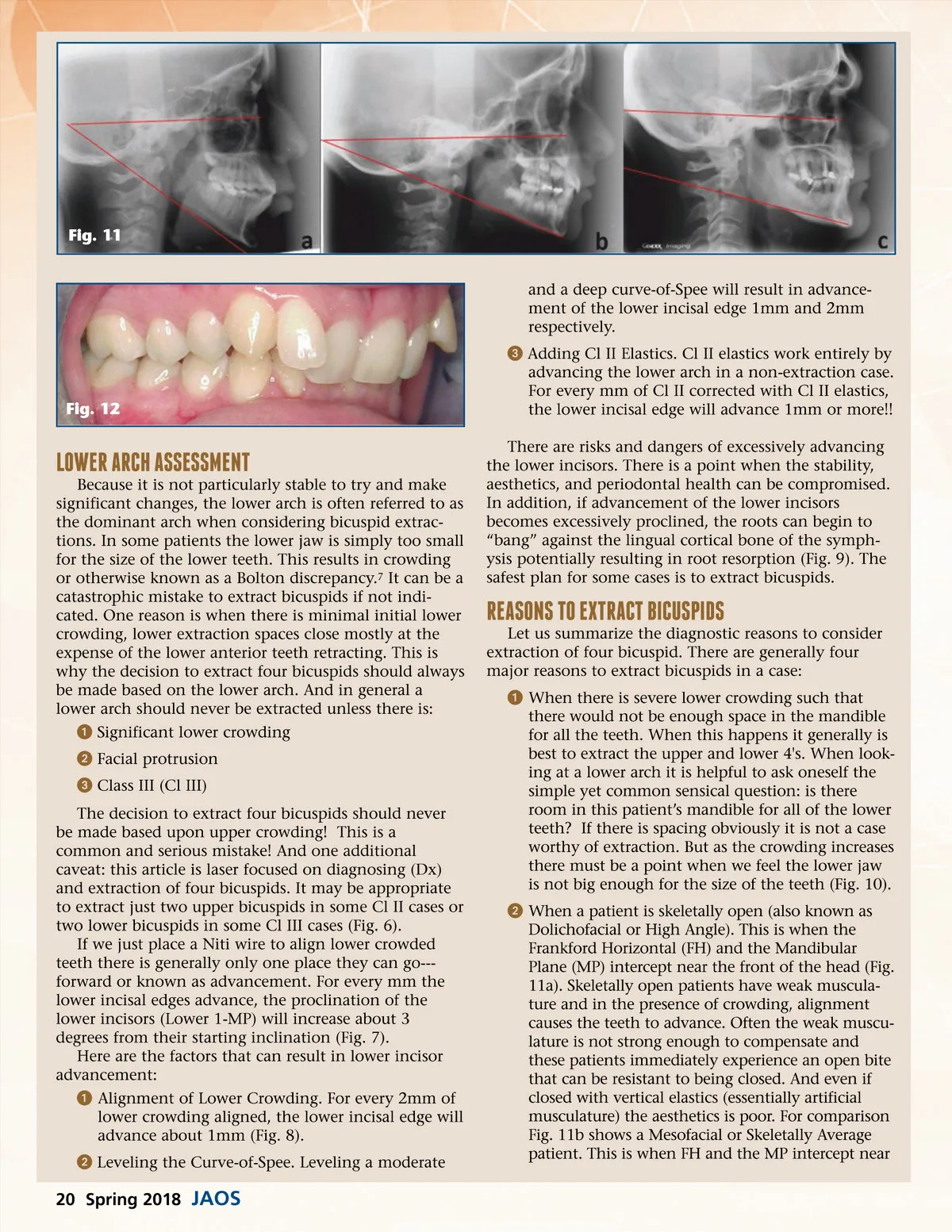
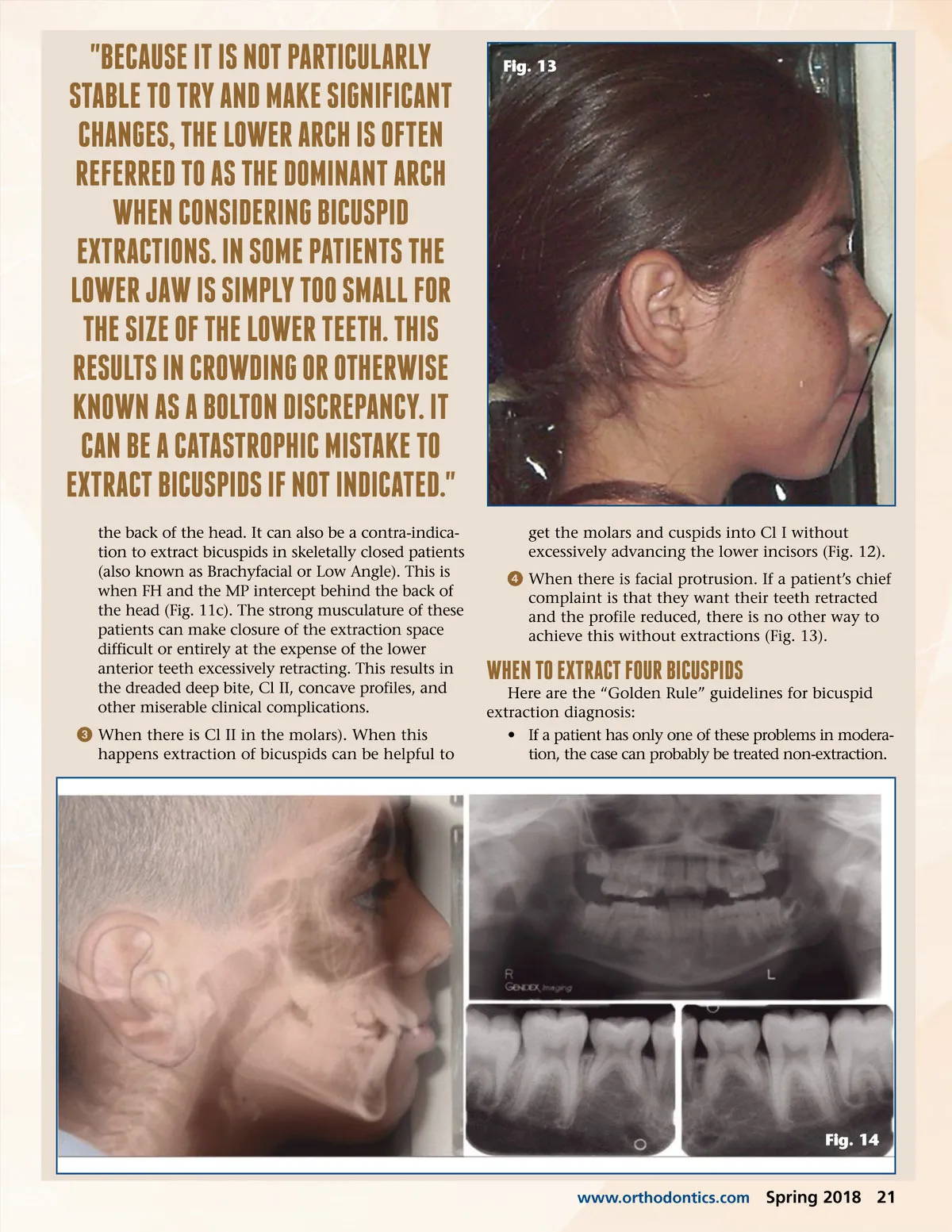
"BECAuSE iT iS noT PARTiCulARlY STABlE To TRY AnD MAkE SignifiCAnT ChAngES, ThE lowER ARCh iS ofTEn REfERRED To AS ThE DoMinAnT ARCh whEn ConSiDERing BiCuSPiD EXTRACTionS. in SoME PATiEnTS ThE lowER jAw iS SiMPlY Too SMAll foR ThE SizE of ThE lowER TEETh. ThiS RESulTS in CRowDing oR oThERwiSE known AS A BolTon DiSCREPAnCY. iT CAn BE A CATASTRoPhiC MiSTAkE To EXTRACT BiCuSPiDS if noT inDiCATED." the back of the head. It can also be a contra-indica-tion to extract bicuspids in skeletally closed patients (also known as Brachyfacial or Low Angle). This is when FH and the MP intercept behind the back of the head (Fig. 11c). The strong musculature of these patients can make closure of the extraction space difficult or entirely at the expense of the lower anterior teeth excessively retracting. This results in the dreaded deep bite, Cl II, concave profiles, and other miserable clinical complications. ᕣ When there is Cl II in the molars). When this happens extraction of bicuspids can be helpful to Fig. 13 get the molars and cuspids into Cl I without excessively advancing the lower incisors (Fig. 12). ᕤ When there is facial protrusion. If a patient’s chief complaint is that they want their teeth retracted and the profile reduced, there is no other way to achieve this without extractions (Fig. 13). whEn To EXTRACT fouR BiCuSPiDS Here are the “Golden Rule” guidelines for bicuspid extraction diagnosis: • If a patient has only one of these problems in modera-tion, the case can probably be treated non-extraction. Fig. 14 www.orthodontics.com Spring 2018 21
Journal of the American Orthodontic Society Spring 2018: Page 21