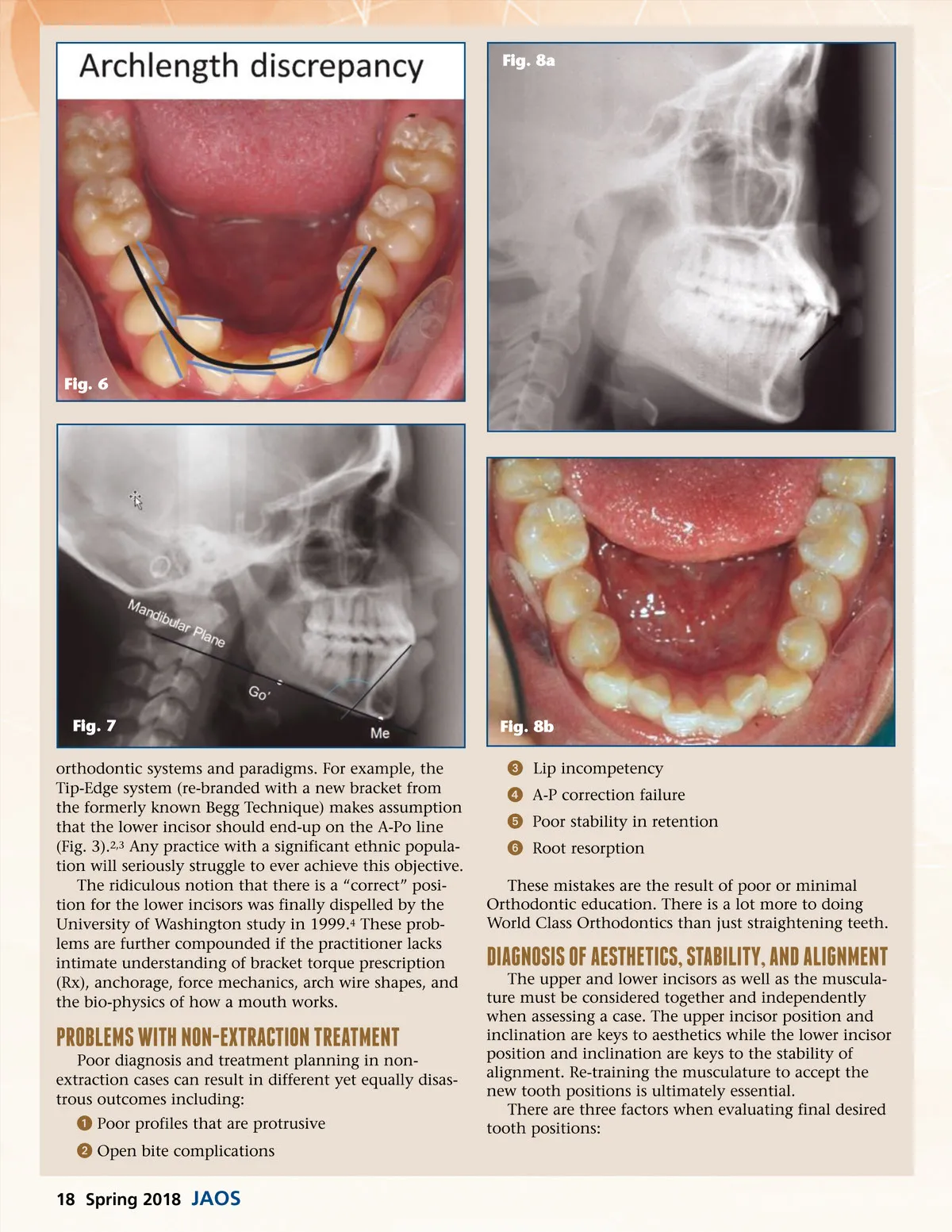
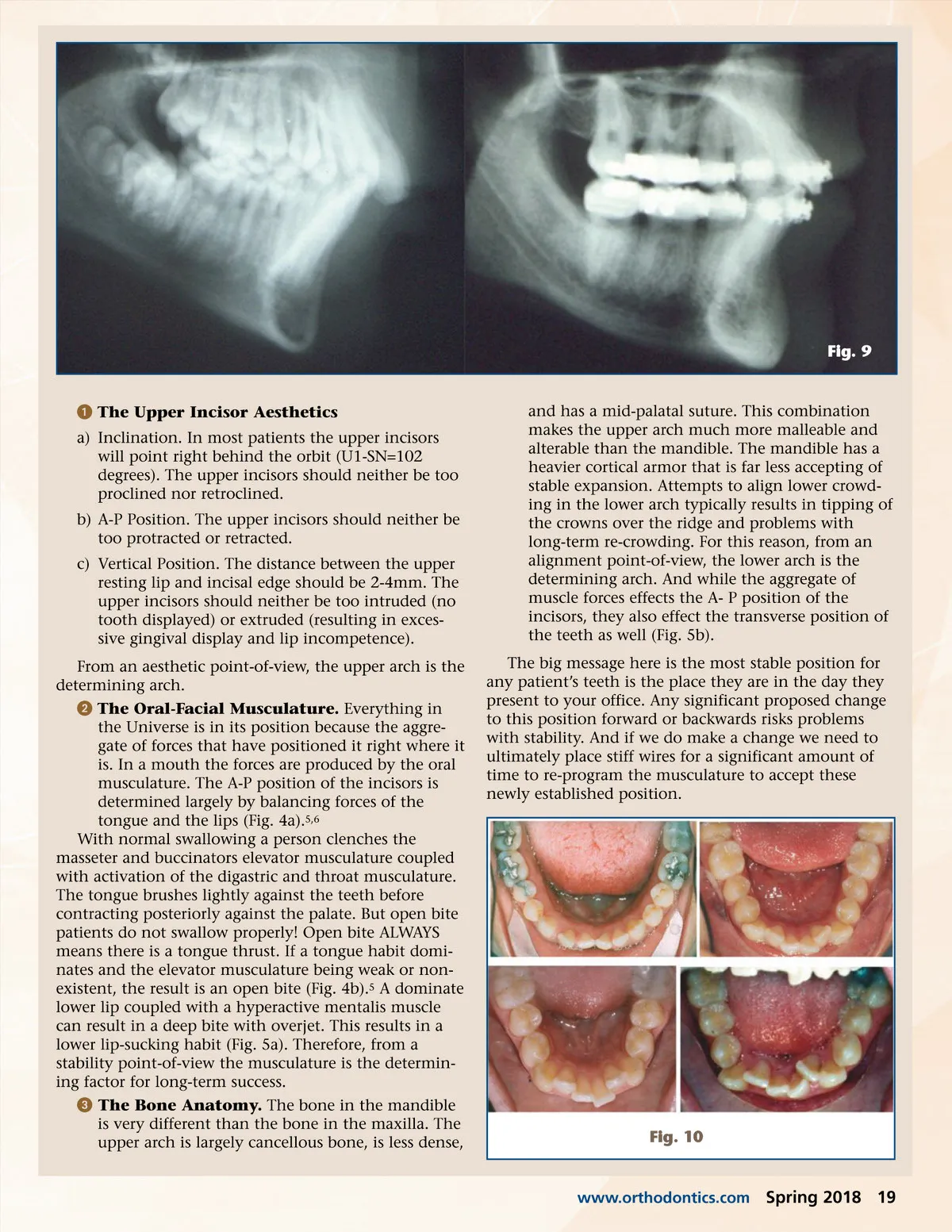
Fig. 9 ᕡ The Upper Incisor Aesthetics a) Inclination. In most patients the upper incisors will point right behind the orbit (U1-SN=102 degrees). The upper incisors should neither be too proclined nor retroclined. b) A-P Position. The upper incisors should neither be too protracted or retracted. c) Vertical Position. The distance between the upper resting lip and incisal edge should be 2-4mm. The upper incisors should neither be too intruded (no tooth displayed) or extruded (resulting in exces-sive gingival display and lip incompetence). From an aesthetic point-of-view, the upper arch is the determining arch. ᕢ The Oral-Facial Musculature. Everything in the Universe is in its position because the aggre-gate of forces that have positioned it right where it is. In a mouth the forces are produced by the oral musculature. The A-P position of the incisors is determined largely by balancing forces of the tongue and the lips (Fig. 4a). 5,6 With normal swallowing a person clenches the masseter and buccinators elevator musculature coupled with activation of the digastric and throat musculature. The tongue brushes lightly against the teeth before contracting posteriorly against the palate. But open bite patients do not swallow properly! Open bite ALWAYS means there is a tongue thrust. If a tongue habit domi-nates and the elevator musculature being weak or non-existent, the result is an open bite (Fig. 4b). 5 A dominate lower lip coupled with a hyperactive mentalis muscle can result in a deep bite with overjet. This results in a lower lip-sucking habit (Fig. 5a). Therefore, from a stability point-of-view the musculature is the determin-ing factor for long-term success. ᕣ The Bone Anatomy. The bone in the mandible is very different than the bone in the maxilla. The upper arch is largely cancellous bone, is less dense, and has a mid-palatal suture. This combination makes the upper arch much more malleable and alterable than the mandible. The mandible has a heavier cortical armor that is far less accepting of stable expansion. Attempts to align lower crowd-ing in the lower arch typically results in tipping of the crowns over the ridge and problems with long-term re-crowding. For this reason, from an alignment point-of-view, the lower arch is the determining arch. And while the aggregate of muscle forces effects the A-P position of the incisors, they also effect the transverse position of the teeth as well (Fig. 5b). The big message here is the most stable position for any patient’s teeth is the place they are in the day they present to your office. Any significant proposed change to this position forward or backwards risks problems with stability. And if we do make a change we need to ultimately place stiff wires for a significant amount of time to re-program the musculature to accept these newly established position. Fig. 10 www.orthodontics.com Spring 2018 19
Journal of the American Orthodontic Society Spring 2018: Page 19