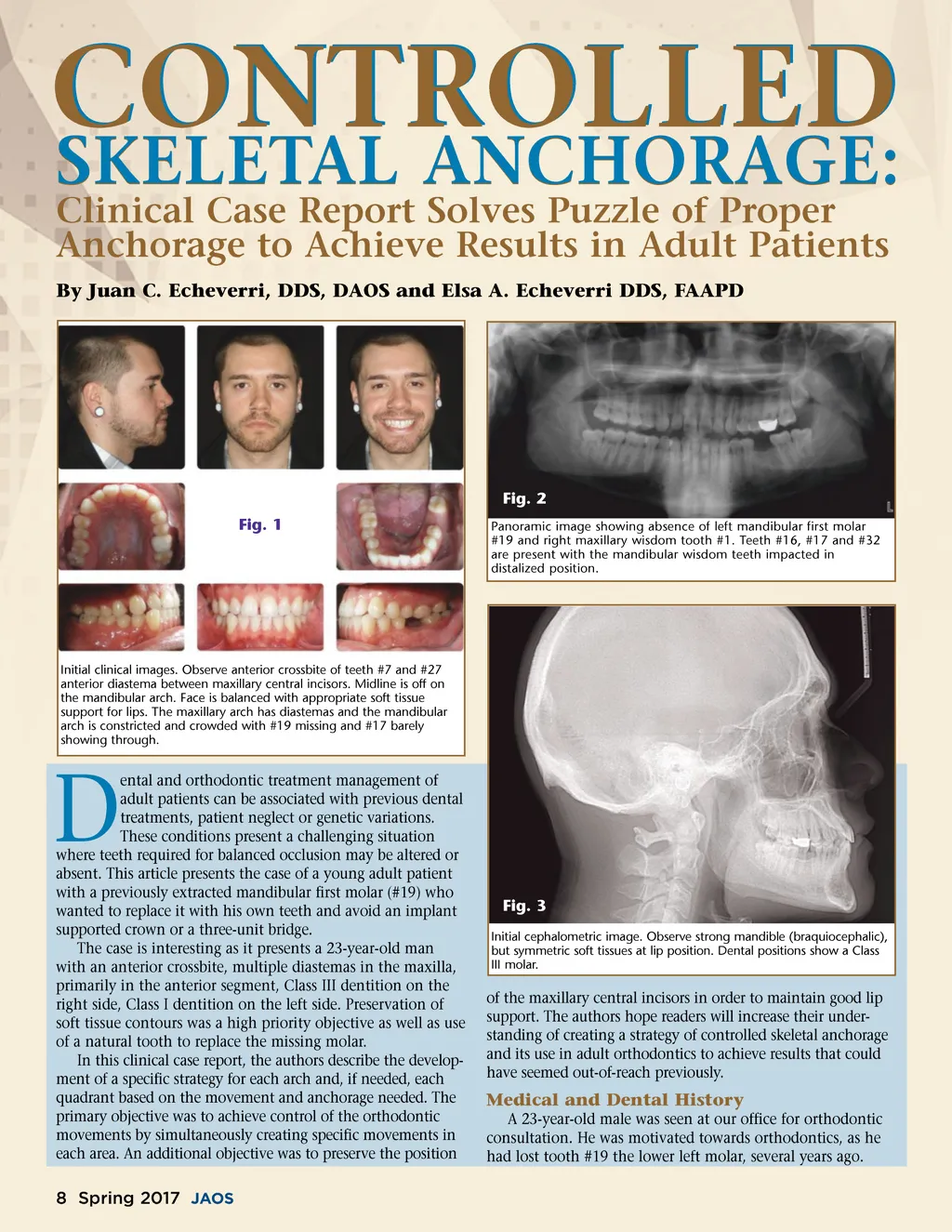
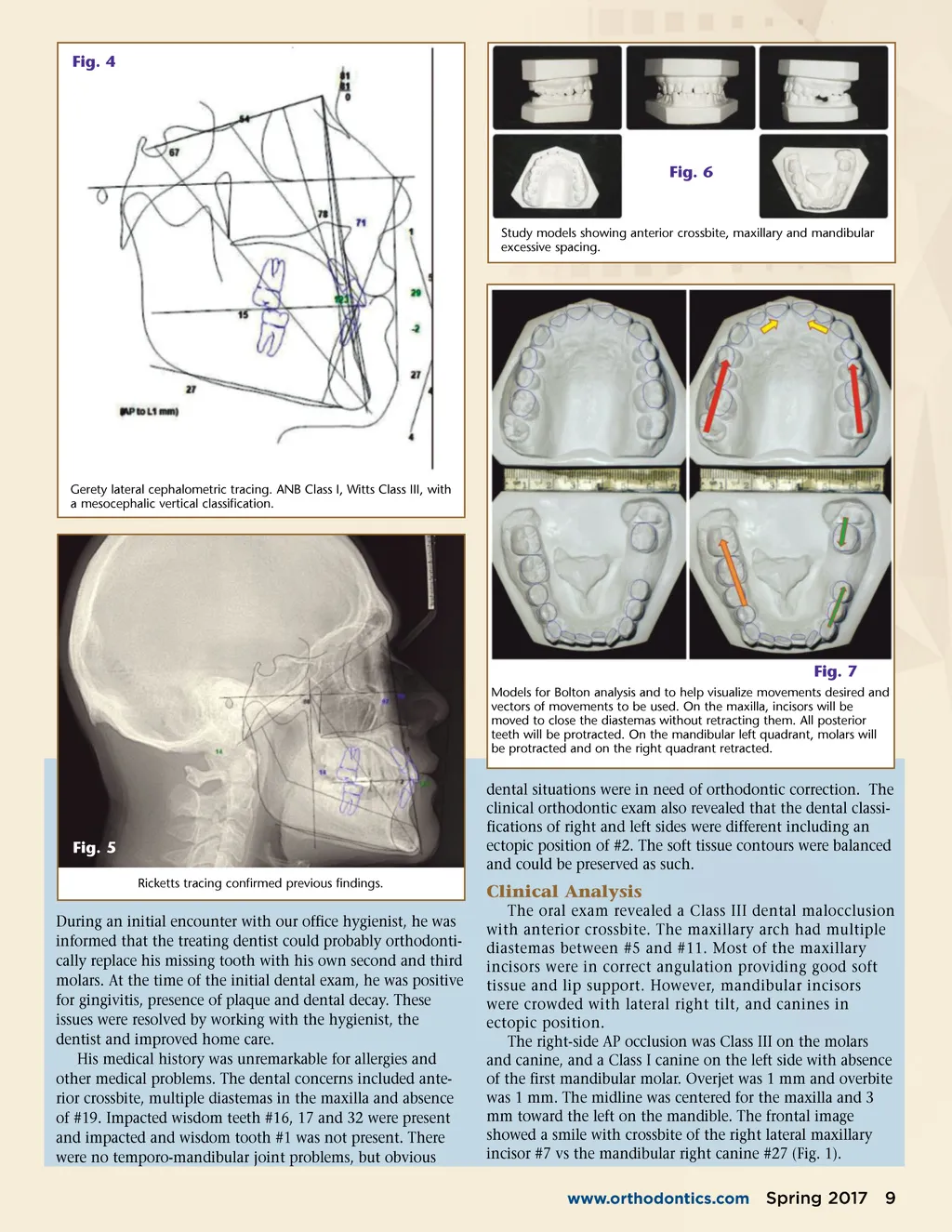
Fig. 4 Fig. 6 Study models showing anterior crossbite, maxillary and mandibular excessive spacing. Gerety lateral cephalometric tracing. ANB Class I, Witts Class III, with a mesocephalic vertical classification. Fig. 7 Models for Bolton analysis and to help visualize movements desired and vectors of movements to be used. On the maxilla, incisors will be moved to close the diastemas without retracting them. All posterior teeth will be protracted. On the mandibular left quadrant, molars will be protracted and on the right quadrant retracted. Fig. 5 Ricketts tracing confirmed previous findings. dental situations were in need of orthodontic correction. The clinical orthodontic exam also revealed that the dental classi-fications of right and left sides were different including an ectopic position of #2. The soft tissue contours were balanced and could be preserved as such. Clinical Analysis The oral exam revealed a Class III dental malocclusion with anterior crossbite. The maxillary arch had multiple diastemas between #5 and #11. Most of the maxillary incisors were in correct angulation providing good soft tissue and lip support. However, mandibular incisors were crowded with lateral right tilt, and canines in ectopic position. The right-side AP occlusion was Class III on the molars and canine, and a Class I canine on the left side with absence of the first mandibular molar. Overjet was 1 mm and overbite was 1 mm. The midline was centered for the maxilla and 3 mm toward the left on the mandible. The frontal image showed a smile with crossbite of the right lateral maxillary incisor #7 vs the mandibular right canine #27 (Fig. 1). www.orthodontics.com During an initial encounter with our office hygienist, he was informed that the treating dentist could probably orthodonti-cally replace his missing tooth with his own second and third molars. At the time of the initial dental exam, he was positive for gingivitis, presence of plaque and dental decay. These issues were resolved by working with the hygienist, the dentist and improved home care. His medical history was unremarkable for allergies and other medical problems. The dental concerns included ante-rior crossbite, multiple diastemas in the maxilla and absence of #19. Impacted wisdom teeth #16, 17 and 32 were present and impacted and wisdom tooth #1 was not present. There were no temporo-mandibular joint problems, but obvious Spring 2017 9
Journal of the American Orthodontic Society Spring 2017: Page 9