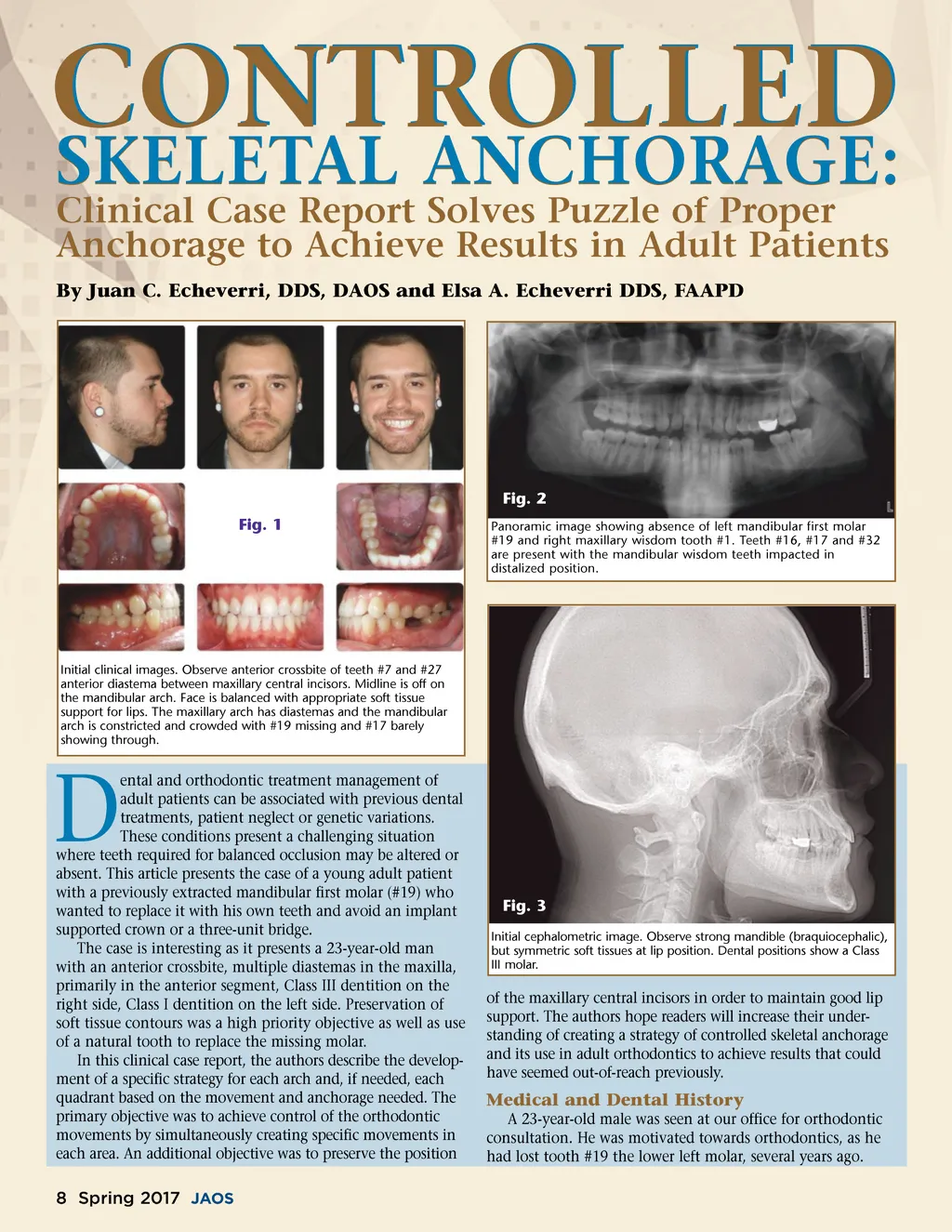
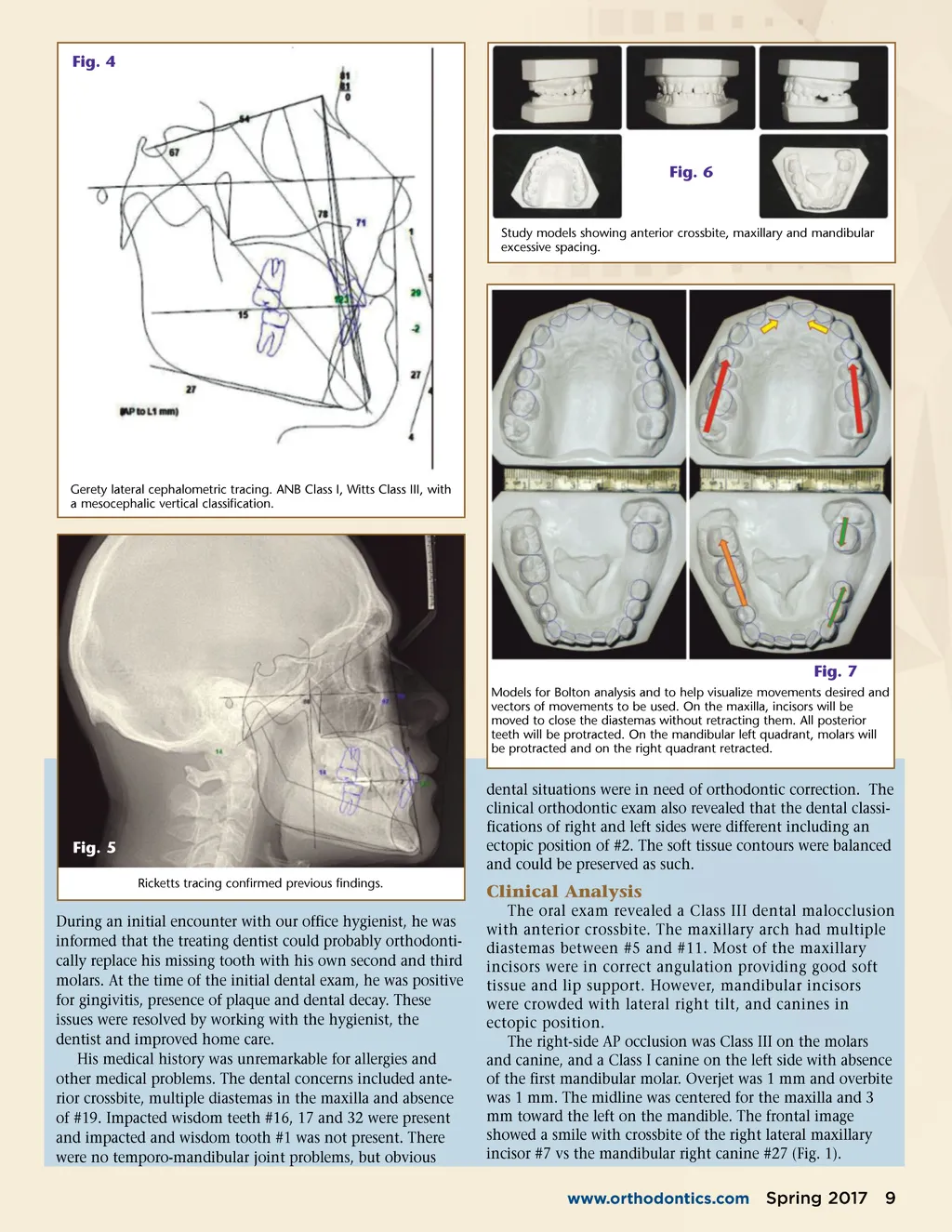
CONTROLLED SKELETAL ANCHORAGE: Clinical Case Report Solves Puzzle of Proper Anchorage to Achieve Results in Adult Patients By Juan C. Echeverri, DDS, DAOS and Elsa A. Echeverri DDS, FAAPD Fig. 2 Fig. 1 Panoramic image showing absence of left mandibular first molar #19 and right maxillary wisdom tooth #1. Teeth #16, #17 and #32 are present with the mandibular wisdom teeth impacted in distalized position. Initial clinical images. Observe anterior crossbite of teeth #7 and #27 anterior diastema between maxillary central incisors. Midline is off on the mandibular arch. Face is balanced with appropriate soft tissue support for lips. The maxillary arch has diastemas and the mandibular arch is constricted and crowded with #19 missing and #17 barely showing through. D ental and orthodontic treatment management of adult patients can be associated with previous dental treatments, patient neglect or genetic variations. These conditions present a challenging situation where teeth required for balanced occlusion may be altered or absent. This article presents the case of a young adult patient with a previously extracted mandibular first molar (#19) who wanted to replace it with his own teeth and avoid an implant supported crown or a three-unit bridge. The case is interesting as it presents a 23-year-old man with an anterior crossbite, multiple diastemas in the maxilla, primarily in the anterior segment, Class III dentition on the right side, Class I dentition on the left side. Preservation of soft tissue contours was a high priority objective as well as use of a natural tooth to replace the missing molar. In this clinical case report, the authors describe the develop-ment of a specific strategy for each arch and, if needed, each quadrant based on the movement and anchorage needed. The primary objective was to achieve control of the orthodontic movements by simultaneously creating specific movements in each area. An additional objective was to preserve the position Fig. 3 Initial cephalometric image. Observe strong mandible (braquiocephalic), but symmetric soft tissues at lip position. Dental positions show a Class III molar. of the maxillary central incisors in order to maintain good lip support. The authors hope readers will increase their under-standing of creating a strategy of controlled skeletal anchorage and its use in adult orthodontics to achieve results that could have seemed out-of-reach previously. Medical and Dental History A 23-year-old male was seen at our office for orthodontic consultation. He was motivated towards orthodontics, as he had lost tooth #19 the lower left molar, several years ago. 8 Spring 2017 JAOS
Journal of the American Orthodontic Society Spring 2017: Page 8