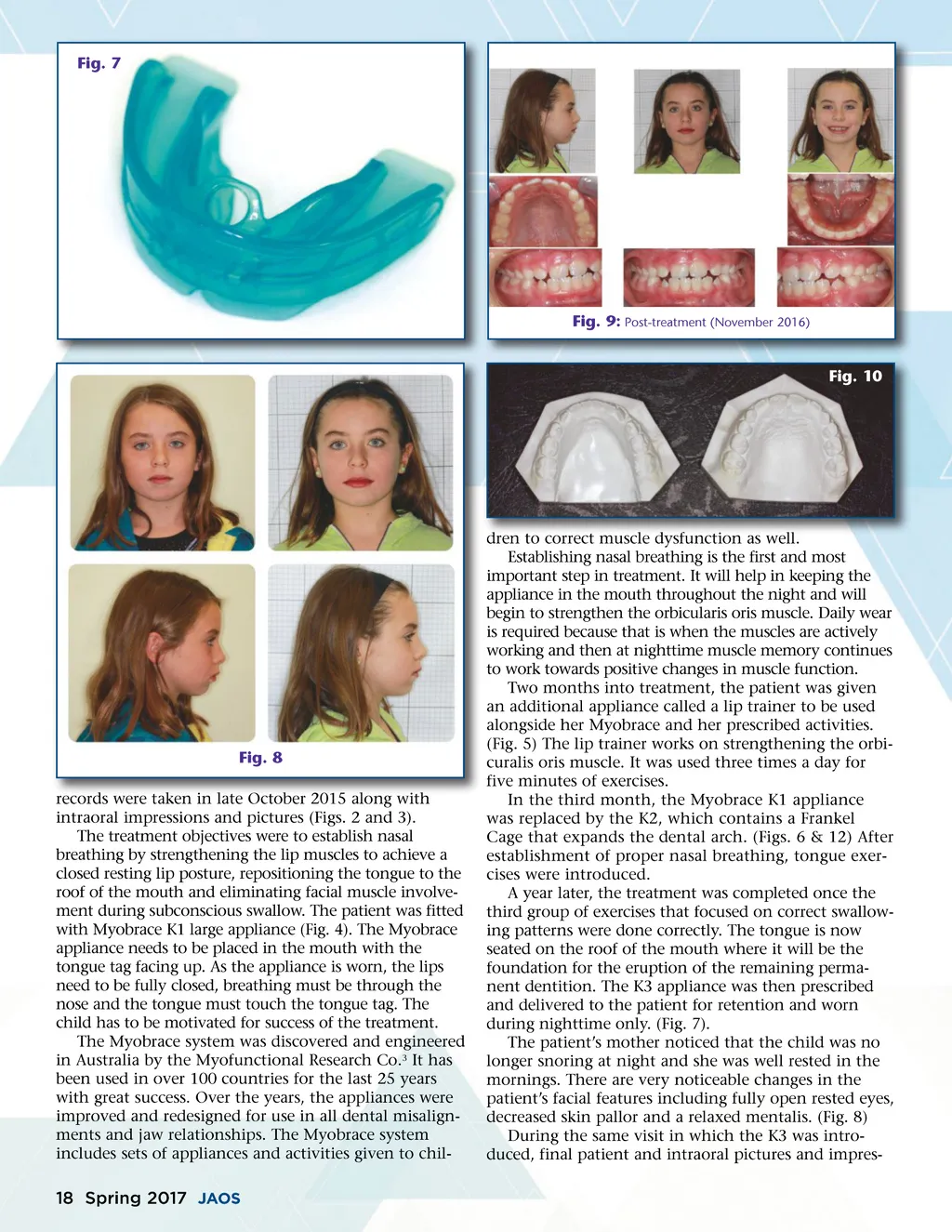
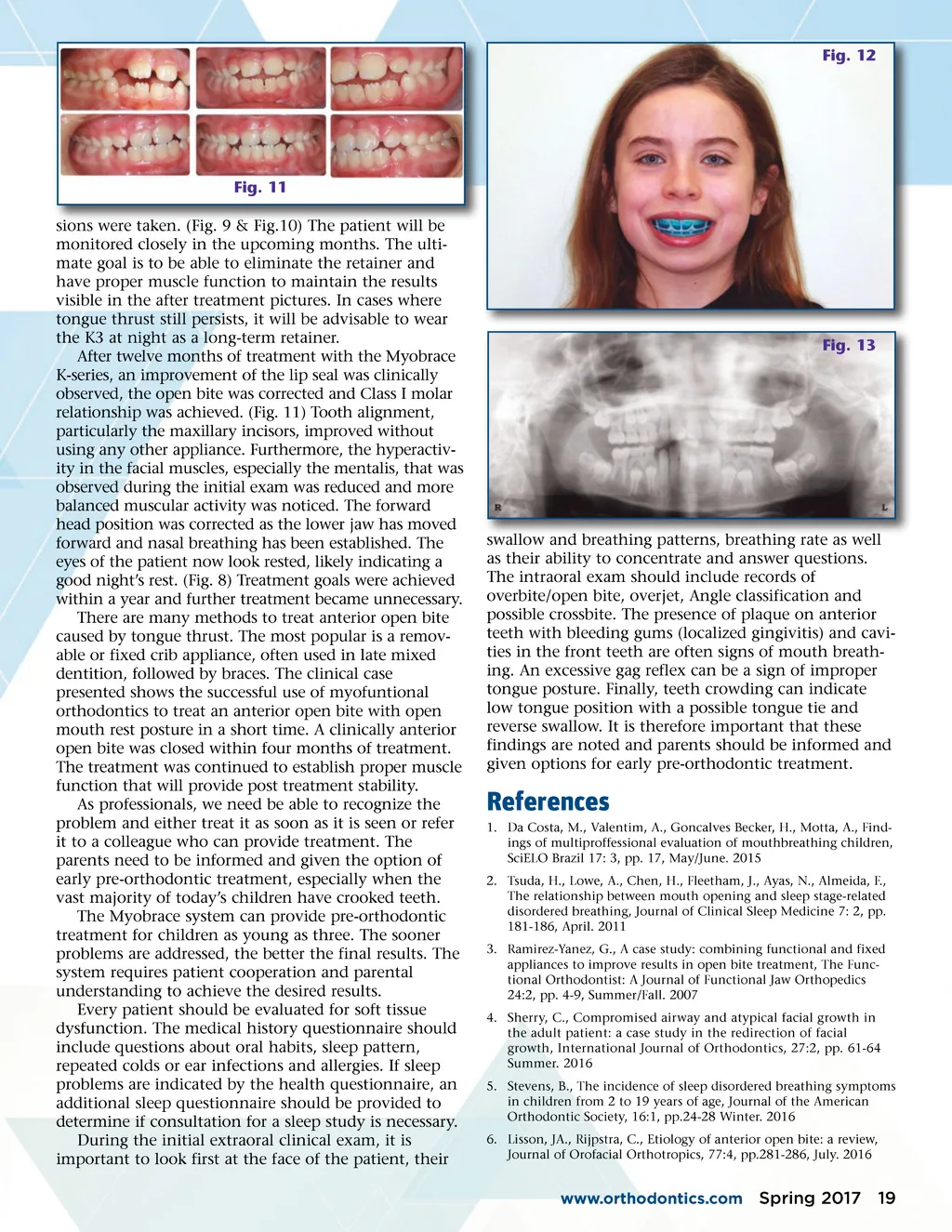
Fig. 12 Fig. 11 sions were taken. (Fig. 9 & Fig.10) The patient will be monitored closely in the upcoming months. The ulti-mate goal is to be able to eliminate the retainer and have proper muscle function to maintain the results visible in the after treatment pictures. In cases where tongue thrust still persists, it will be advisable to wear the K3 at night as a long-term retainer. After twelve months of treatment with the Myobrace K-series, an improvement of the lip seal was clinically observed, the open bite was corrected and Class I molar relationship was achieved. (Fig. 11) Tooth alignment, particularly the maxillary incisors, improved without using any other appliance. Furthermore, the hyperactiv-ity in the facial muscles, especially the mentalis, that was observed during the initial exam was reduced and more balanced muscular activity was noticed. The forward head position was corrected as the lower jaw has moved forward and nasal breathing has been established. The eyes of the patient now look rested, likely indicating a good night’s rest. (Fig. 8) Treatment goals were achieved within a year and further treatment became unnecessary. There are many methods to treat anterior open bite caused by tongue thrust. The most popular is a remov-able or fixed crib appliance, often used in late mixed dentition, followed by braces. The clinical case presented shows the successful use of myofuntional orthodontics to treat an anterior open bite with open mouth rest posture in a short time. A clinically anterior open bite was closed within four months of treatment. The treatment was continued to establish proper muscle function that will provide post treatment stability. As professionals, we need be able to recognize the problem and either treat it as soon as it is seen or refer it to a colleague who can provide treatment. The parents need to be informed and given the option of early pre-orthodontic treatment, especially when the vast majority of today’s children have crooked teeth. The Myobrace system can provide pre-orthodontic treatment for children as young as three. The sooner problems are addressed, the better the final results. The system requires patient cooperation and parental understanding to achieve the desired results. Every patient should be evaluated for soft tissue dysfunction. The medical history questionnaire should include questions about oral habits, sleep pattern, repeated colds or ear infections and allergies. If sleep problems are indicated by the health questionnaire, an additional sleep questionnaire should be provided to determine if consultation for a sleep study is necessary. During the initial extraoral clinical exam, it is important to look first at the face of the patient, their Fig. 13 swallow and breathing patterns, breathing rate as well as their ability to concentrate and answer questions. The intraoral exam should include records of overbite/open bite, overjet, Angle classification and possible crossbite. The presence of plaque on anterior teeth with bleeding gums (localized gingivitis) and cavi-ties in the front teeth are often signs of mouth breath-ing. An excessive gag reflex can be a sign of improper tongue posture. Finally, teeth crowding can indicate low tongue position with a possible tongue tie and reverse swallow. It is therefore important that these findings are noted and parents should be informed and given options for early pre-orthodontic treatment. References 1. Da Costa, M., Valentim, A., Goncalves Becker, H., Motta, A., Find-ings of multiproffessional evaluation of mouthbreathing children, SciELO Brazil 17: 3, pp. 17, May/June. 2015 2. Tsuda, H., Lowe, A., Chen, H., Fleetham, J., Ayas, N., Almeida, F., The relationship between mouth opening and sleep stage-related disordered breathing, Journal of Clinical Sleep Medicine 7: 2, pp. 181-186, April. 2011 3. Ramirez-Yanez, G., A case study: combining functional and fixed appliances to improve results in open bite treatment, The Func-tional Orthodontist: A Journal of Functional Jaw Orthopedics 24:2, pp. 4-9, Summer/Fall. 2007 4. Sherry, C., Compromised airway and atypical facial growth in the adult patient: a case study in the redirection of facial growth, International Journal of Orthodontics, 27:2, pp. 61-64 Summer. 2016 5. Stevens, B., The incidence of sleep disordered breathing symptoms in children from 2 to 19 years of age, Journal of the American Orthodontic Society, 16:1, pp.24-28 Winter. 2016 6. Lisson, JA., Rijpstra, C., Etiology of anterior open bite: a review, Journal of Orofacial Orthotropics, 77:4, pp.281-286, July. 2016 www.orthodontics.com Spring 2017 19
Journal of the American Orthodontic Society Spring 2017: Page 19