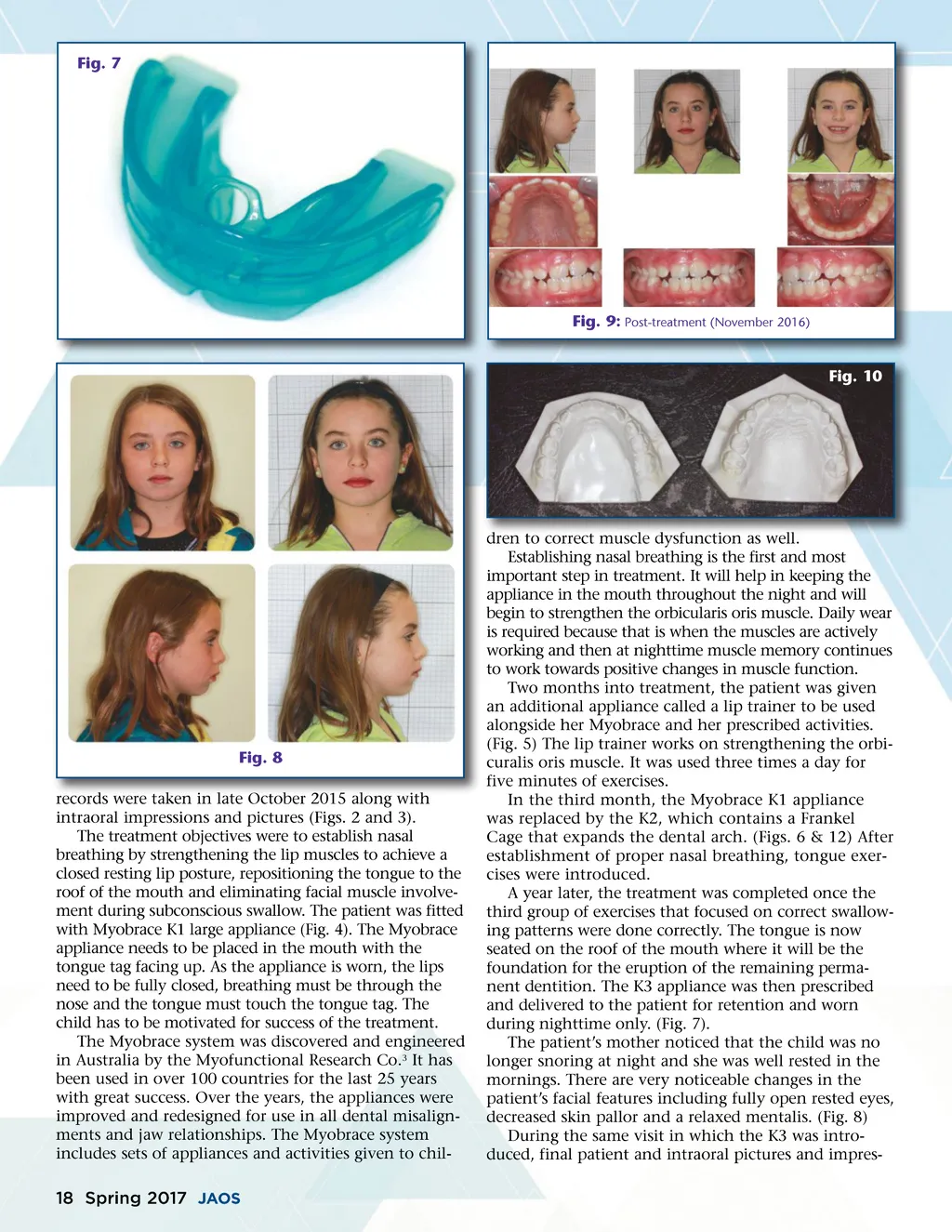
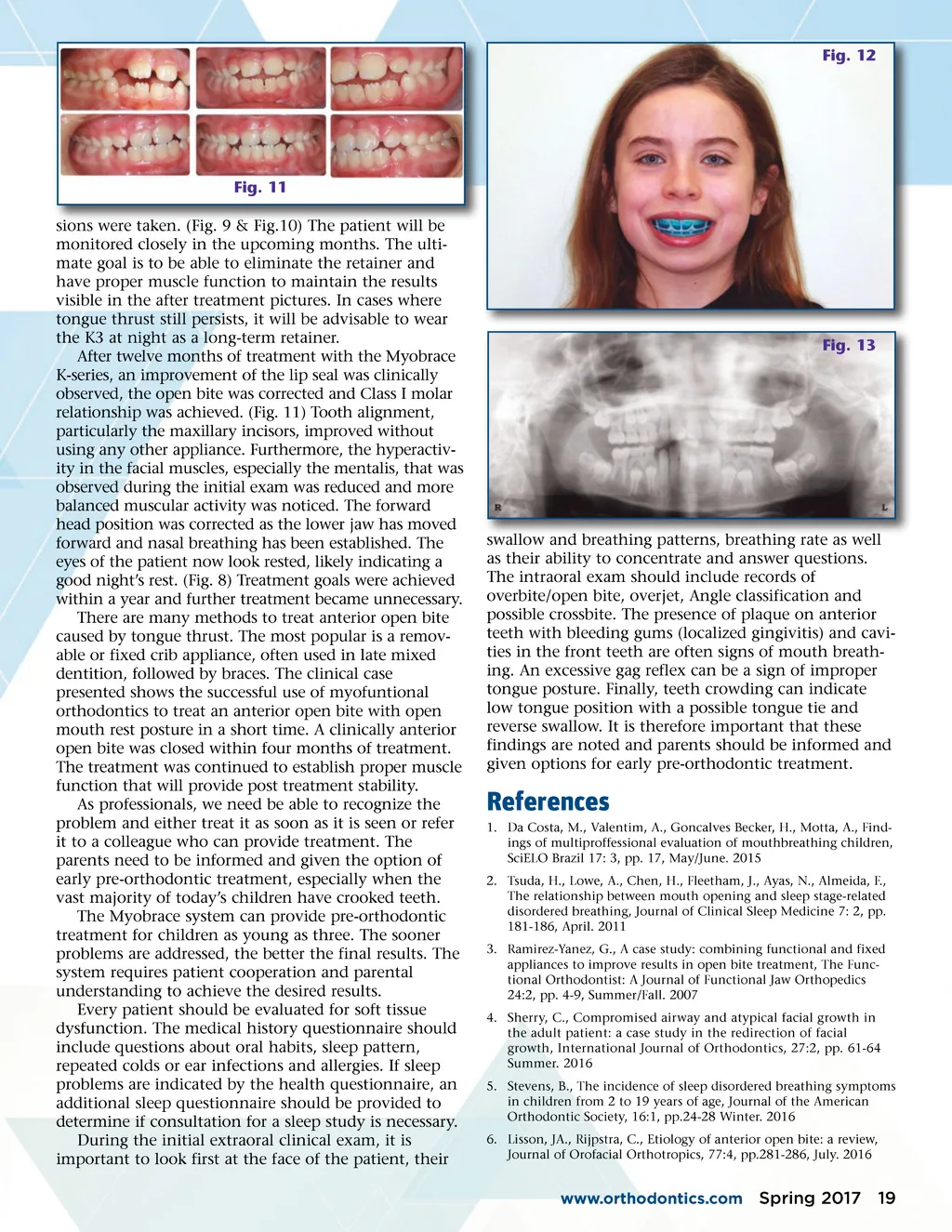
Fig. 7 Fig. 9: Post-treatment (November 2016) Fig. 10 Fig. 8 records were taken in late October 2015 along with intraoral impressions and pictures (Figs. 2 and 3). The treatment objectives were to establish nasal breathing by strengthening the lip muscles to achieve a closed resting lip posture, repositioning the tongue to the roof of the mouth and eliminating facial muscle involve-ment during subconscious swallow. The patient was fitted with Myobrace K1 large appliance (Fig. 4). The Myobrace appliance needs to be placed in the mouth with the tongue tag facing up. As the appliance is worn, the lips need to be fully closed, breathing must be through the nose and the tongue must touch the tongue tag. The child has to be motivated for success of the treatment. The Myobrace system was discovered and engineered in Australia by the Myofunctional Research Co. 3 It has been used in over 100 countries for the last 25 years with great success. Over the years, the appliances were improved and redesigned for use in all dental misalign-ments and jaw relationships. The Myobrace system includes sets of appliances and activities given to chil-dren to correct muscle dysfunction as well. Establishing nasal breathing is the first and most important step in treatment. It will help in keeping the appliance in the mouth throughout the night and will begin to strengthen the orbicularis oris muscle. Daily wear is required because that is when the muscles are actively working and then at nighttime muscle memory continues to work towards positive changes in muscle function. Two months into treatment, the patient was given an additional appliance called a lip trainer to be used alongside her Myobrace and her prescribed activities. (Fig. 5) The lip trainer works on strengthening the orbi-curalis oris muscle. It was used three times a day for five minutes of exercises. In the third month, the Myobrace K1 appliance was replaced by the K2, which contains a Frankel Cage that expands the dental arch. (Figs. 6 & 12) After establishment of proper nasal breathing, tongue exer-cises were introduced. A year later, the treatment was completed once the third group of exercises that focused on correct swallow-ing patterns were done correctly. The tongue is now seated on the roof of the mouth where it will be the foundation for the eruption of the remaining perma-nent dentition. The K3 appliance was then prescribed and delivered to the patient for retention and worn during nighttime only. (Fig. 7). The patient’s mother noticed that the child was no longer snoring at night and she was well rested in the mornings. There are very noticeable changes in the patient’s facial features including fully open rested eyes, decreased skin pallor and a relaxed mentalis. (Fig. 8) During the same visit in which the K3 was intro-duced, final patient and intraoral pictures and impres-18 Spring 2017 JAOS
Journal of the American Orthodontic Society Spring 2017: Page 18