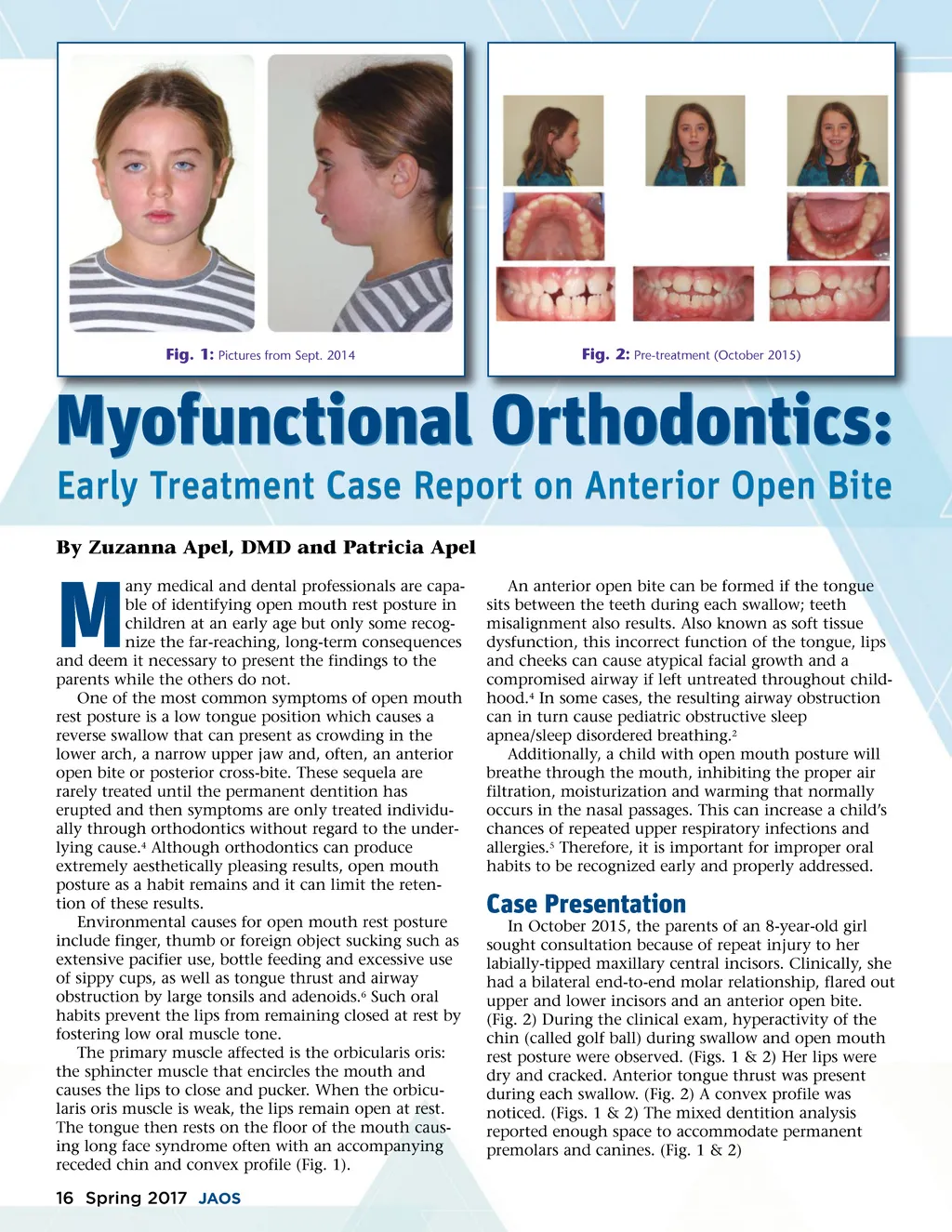
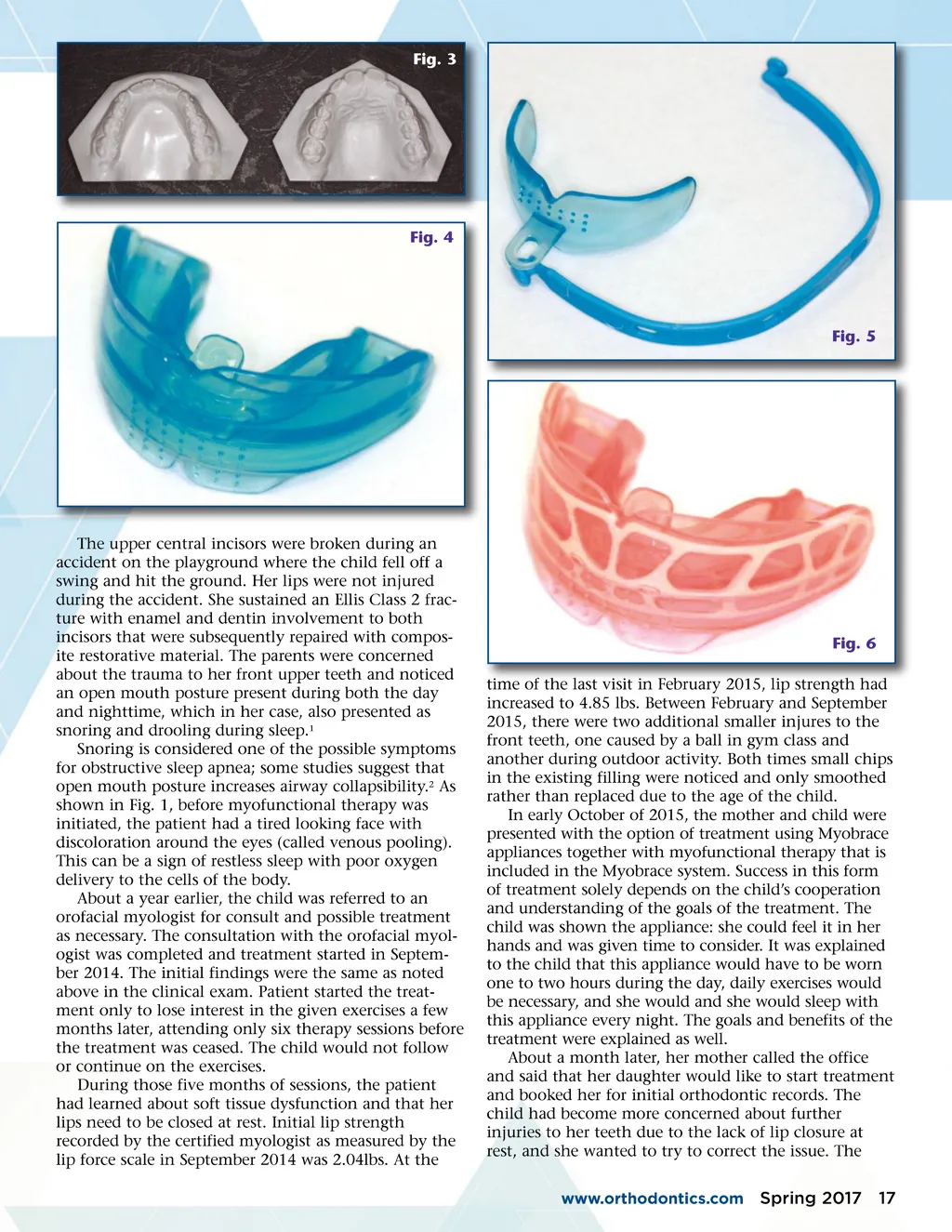
Fig. 3 Fig. 4 Fig. 5 The upper central incisors were broken during an accident on the playground where the child fell off a swing and hit the ground. Her lips were not injured during the accident. She sustained an Ellis Class 2 frac-ture with enamel and dentin involvement to both incisors that were subsequently repaired with compos-ite restorative material. The parents were concerned about the trauma to her front upper teeth and noticed an open mouth posture present during both the day and nighttime, which in her case, also presented as snoring and drooling during sleep. 1 Snoring is considered one of the possible symptoms for obstructive sleep apnea; some studies suggest that open mouth posture increases airway collapsibility. 2 As shown in Fig. 1, before myofunctional therapy was initiated, the patient had a tired looking face with discoloration around the eyes (called venous pooling). This can be a sign of restless sleep with poor oxygen delivery to the cells of the body. About a year earlier, the child was referred to an orofacial myologist for consult and possible treatment as necessary. The consultation with the orofacial myol-ogist was completed and treatment started in Septem-ber 2014. The initial findings were the same as noted above in the clinical exam. Patient started the treat-ment only to lose interest in the given exercises a few months later, attending only six therapy sessions before the treatment was ceased. The child would not follow or continue on the exercises. During those five months of sessions, the patient had learned about soft tissue dysfunction and that her lips need to be closed at rest. Initial lip strength recorded by the certified myologist as measured by the lip force scale in September 2014 was 2.04lbs. At the Fig. 6 time of the last visit in February 2015, lip strength had increased to 4.85 lbs. Between February and September 2015, there were two additional smaller injures to the front teeth, one caused by a ball in gym class and another during outdoor activity. Both times small chips in the existing filling were noticed and only smoothed rather than replaced due to the age of the child. In early October of 2015, the mother and child were presented with the option of treatment using Myobrace appliances together with myofunctional therapy that is included in the Myobrace system. Success in this form of treatment solely depends on the child’s cooperation and understanding of the goals of the treatment. The child was shown the appliance: she could feel it in her hands and was given time to consider. It was explained to the child that this appliance would have to be worn one to two hours during the day, daily exercises would be necessary, and she would and she would sleep with this appliance every night. The goals and benefits of the treatment were explained as well. About a month later, her mother called the office and said that her daughter would like to start treatment and booked her for initial orthodontic records. The child had become more concerned about further injuries to her teeth due to the lack of lip closure at rest, and she wanted to try to correct the issue. The www.orthodontics.com Spring 2017 17
Journal of the American Orthodontic Society Spring 2017: Page 17