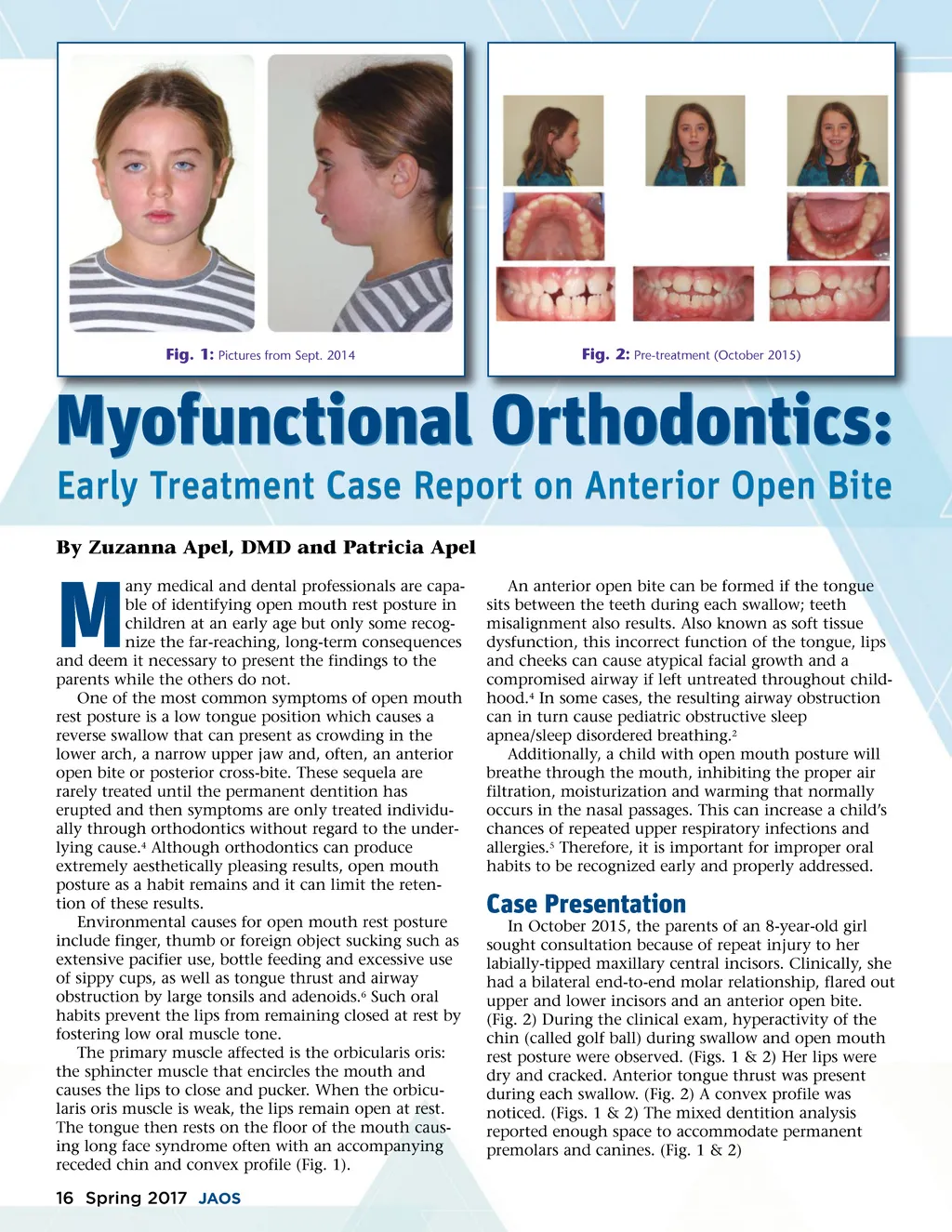
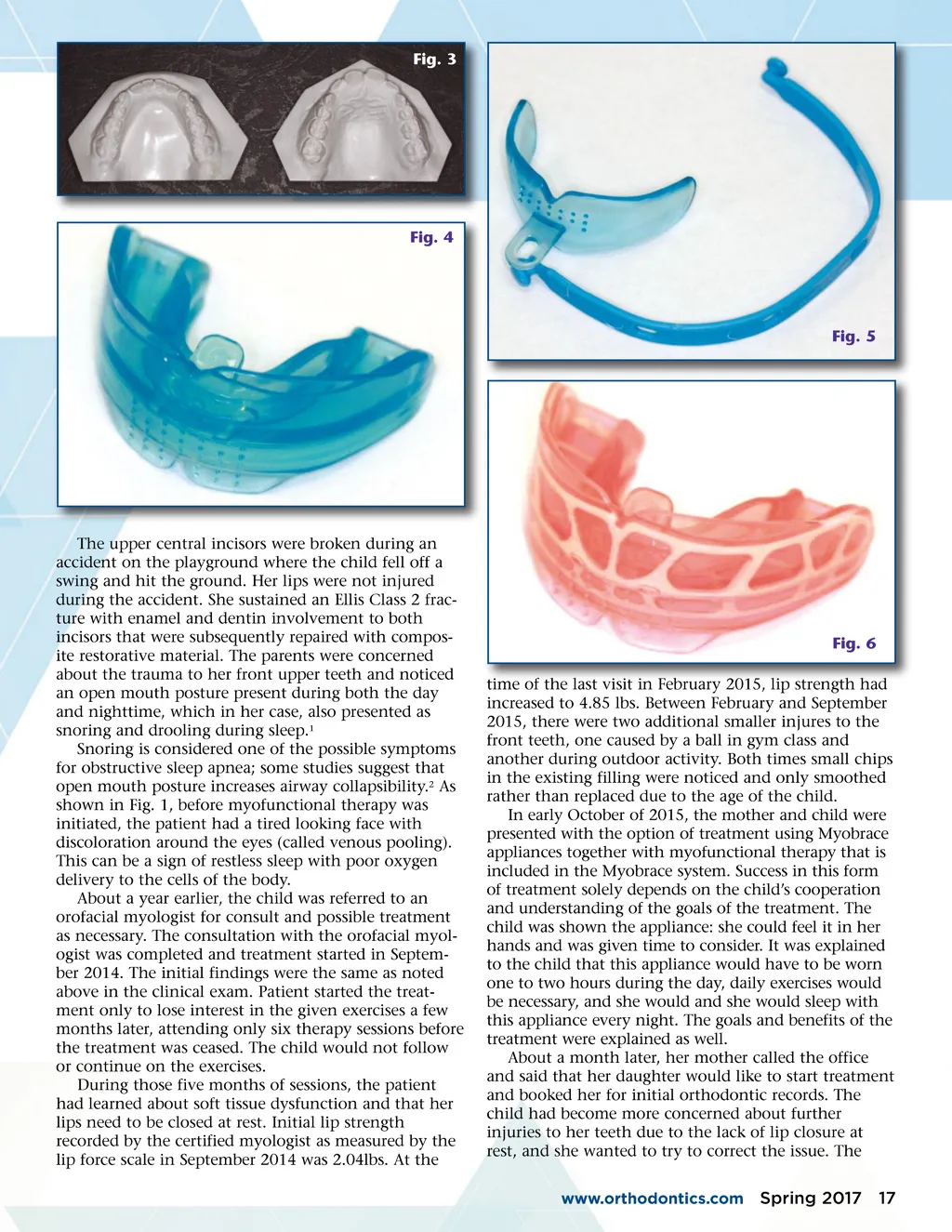
Fig. 1: Pictures from Sept. 2014 Fig. 2: Pre-treatment (October 2015) Myofunctional Orthodontics: Early Treatment Case Report on Anterior Open Bite By Zuzanna Apel, DMD and Patricia Apel any medical and dental professionals are capa-ble of identifying open mouth rest posture in children at an early age but only some recog-nize the far-reaching, long-term consequences and deem it necessary to present the findings to the parents while the others do not. One of the most common symptoms of open mouth rest posture is a low tongue position which causes a reverse swallow that can present as crowding in the lower arch, a narrow upper jaw and, often, an anterior open bite or posterior cross-bite. These sequela are rarely treated until the permanent dentition has erupted and then symptoms are only treated individu-ally through orthodontics without regard to the under-lying cause. 4 Although orthodontics can produce extremely aesthetically pleasing results, open mouth posture as a habit remains and it can limit the reten-tion of these results. Environmental causes for open mouth rest posture include finger, thumb or foreign object sucking such as extensive pacifier use, bottle feeding and excessive use of sippy cups, as well as tongue thrust and airway obstruction by large tonsils and adenoids. 6 Such oral habits prevent the lips from remaining closed at rest by fostering low oral muscle tone. The primary muscle affected is the orbicularis oris: the sphincter muscle that encircles the mouth and causes the lips to close and pucker. When the orbicu-laris oris muscle is weak, the lips remain open at rest. The tongue then rests on the floor of the mouth caus-ing long face syndrome often with an accompanying receded chin and convex profile (Fig. 1). M An anterior open bite can be formed if the tongue sits between the teeth during each swallow; teeth misalignment also results. Also known as soft tissue dysfunction, this incorrect function of the tongue, lips and cheeks can cause atypical facial growth and a compromised airway if left untreated throughout child-hood. 4 In some cases, the resulting airway obstruction can in turn cause pediatric obstructive sleep apnea/sleep disordered breathing. 2 Additionally, a child with open mouth posture will breathe through the mouth, inhibiting the proper air filtration, moisturization and warming that normally occurs in the nasal passages. This can increase a child’s chances of repeated upper respiratory infections and allergies. 5 Therefore, it is important for improper oral habits to be recognized early and properly addressed. Case Presentation In October 2015, the parents of an 8-year-old girl sought consultation because of repeat injury to her labially-tipped maxillary central incisors. Clinically, she had a bilateral end-to-end molar relationship, flared out upper and lower incisors and an anterior open bite. (Fig. 2) During the clinical exam, hyperactivity of the chin (called golf ball) during swallow and open mouth rest posture were observed. (Figs. 1 & 2) Her lips were dry and cracked. Anterior tongue thrust was present during each swallow. (Fig. 2) A convex profile was noticed. (Figs. 1 & 2) The mixed dentition analysis reported enough space to accommodate permanent premolars and canines. (Fig. 1 & 2) 16 Spring 2017 JAOS
Journal of the American Orthodontic Society Spring 2017: Page 16