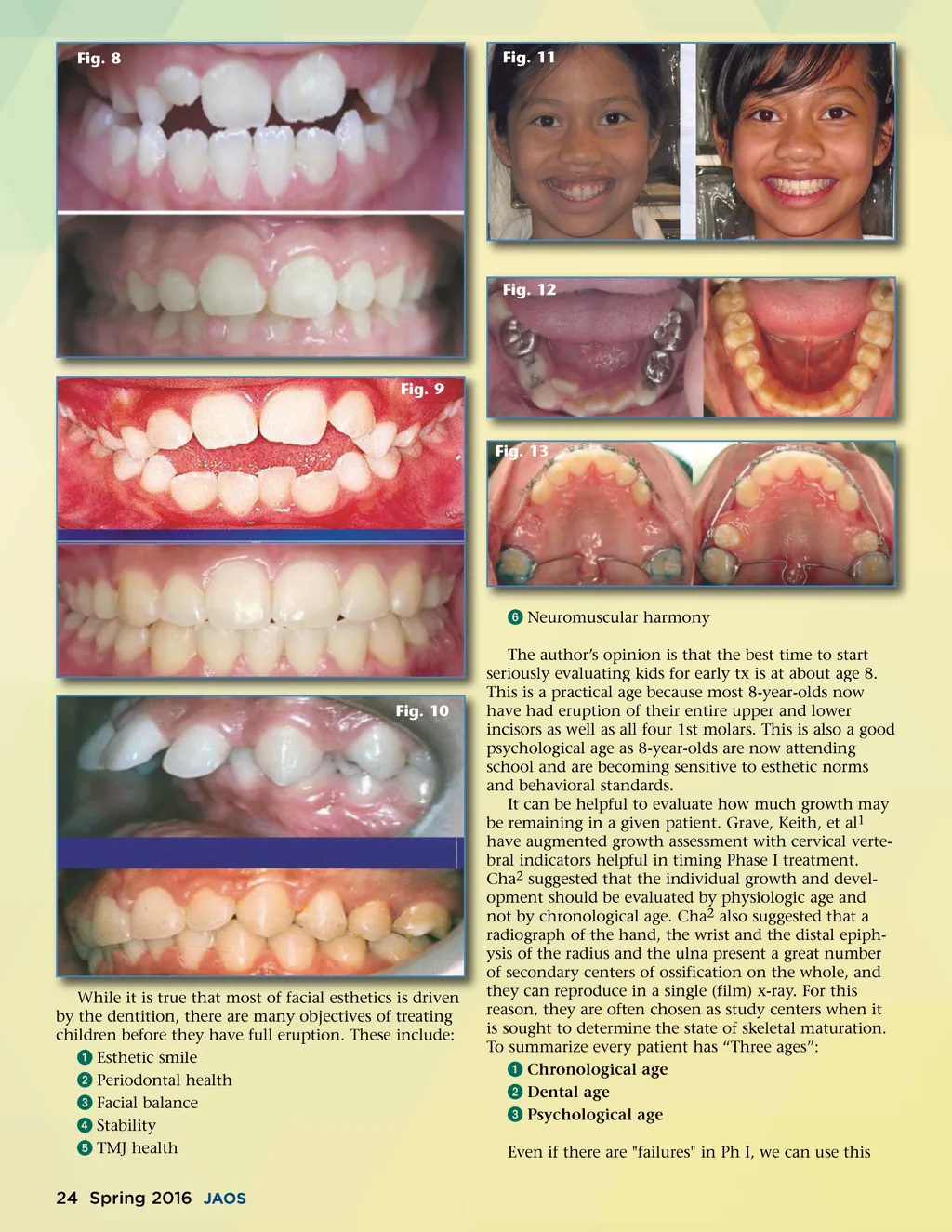
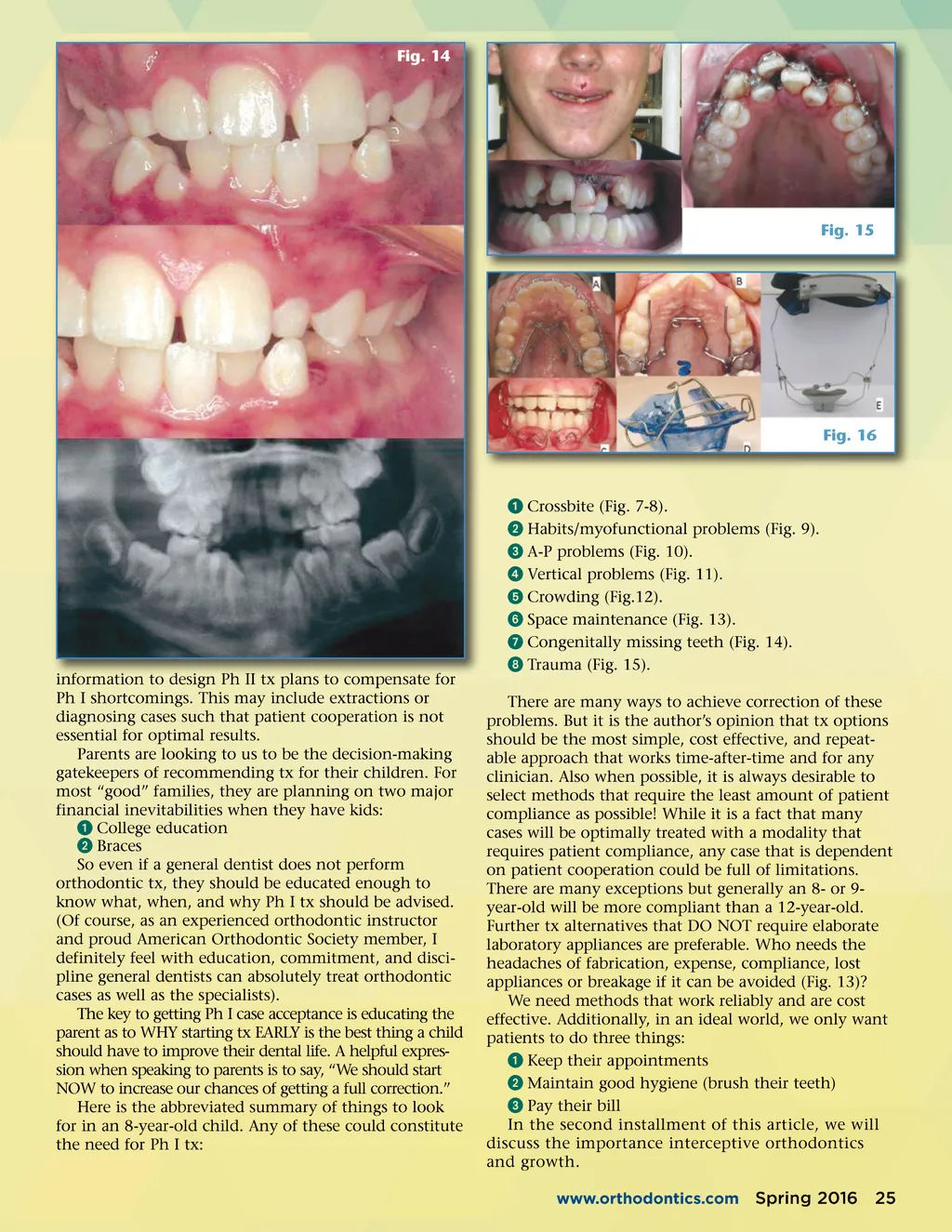
Fig. 14 Fig. 15 Fig. 16 information to design Ph II tx plans to compensate for Ph I shortcomings. This may include extractions or diagnosing cases such that patient cooperation is not essential for optimal results. Parents are looking to us to be the decision-making gatekeepers of recommending tx for their children. For most “good” families, they are planning on two major financial inevitabilities when they have kids: ᕡ College education ᕢ Braces So even if a general dentist does not perform orthodontic tx, they should be educated enough to know what, when, and why Ph I tx should be advised. (Of course, as an experienced orthodontic instructor and proud American Orthodontic Society member, I definitely feel with education, commitment, and disci-pline general dentists can absolutely treat orthodontic cases as well as the specialists). The key to getting Ph I case acceptance is educating the parent as to WHY starting tx EARLY is the best thing a child should have to improve their dental life. A helpful expres-sion when speaking to parents is to say, “We should start NOW to increase our chances of getting a full correction.” Here is the abbreviated summary of things to look for in an 8-year-old child. Any of these could constitute the need for Ph I tx: ᕡ Crossbite (Fig. 7-8). ᕢ Habits/myofunctional problems (Fig. 9). ᕣ A-P problems (Fig. 10). ᕤ Vertical problems (Fig. 11). ᕥ Crowding (Fig.12). ᕦ Space maintenance (Fig. 13). ᕧ Congenitally missing teeth (Fig. 14). ᕨ Trauma (Fig. 15). There are many ways to achieve correction of these problems. But it is the author’s opinion that tx options should be the most simple, cost effective, and repeat-able approach that works time-after-time and for any clinician. Also when possible, it is always desirable to select methods that require the least amount of patient compliance as possible! While it is a fact that many cases will be optimally treated with a modality that requires patient compliance, any case that is dependent on patient cooperation could be full of limitations. There are many exceptions but generally an 8-or 9-year-old will be more compliant than a 12-year-old. Further tx alternatives that DO NOT require elaborate laboratory appliances are preferable. Who needs the headaches of fabrication, expense, compliance, lost appliances or breakage if it can be avoided (Fig. 13)? We need methods that work reliably and are cost effective. Additionally, in an ideal world, we only want patients to do three things: ᕡ Keep their appointments ᕢ Maintain good hygiene (brush their teeth) ᕣ Pay their bill In the second installment of this article, we will discuss the importance interceptive orthodontics and growth. www.orthodontics.com Spring 2016 25
Journal of the American Orthodontic Society Spring 2016: Page 25