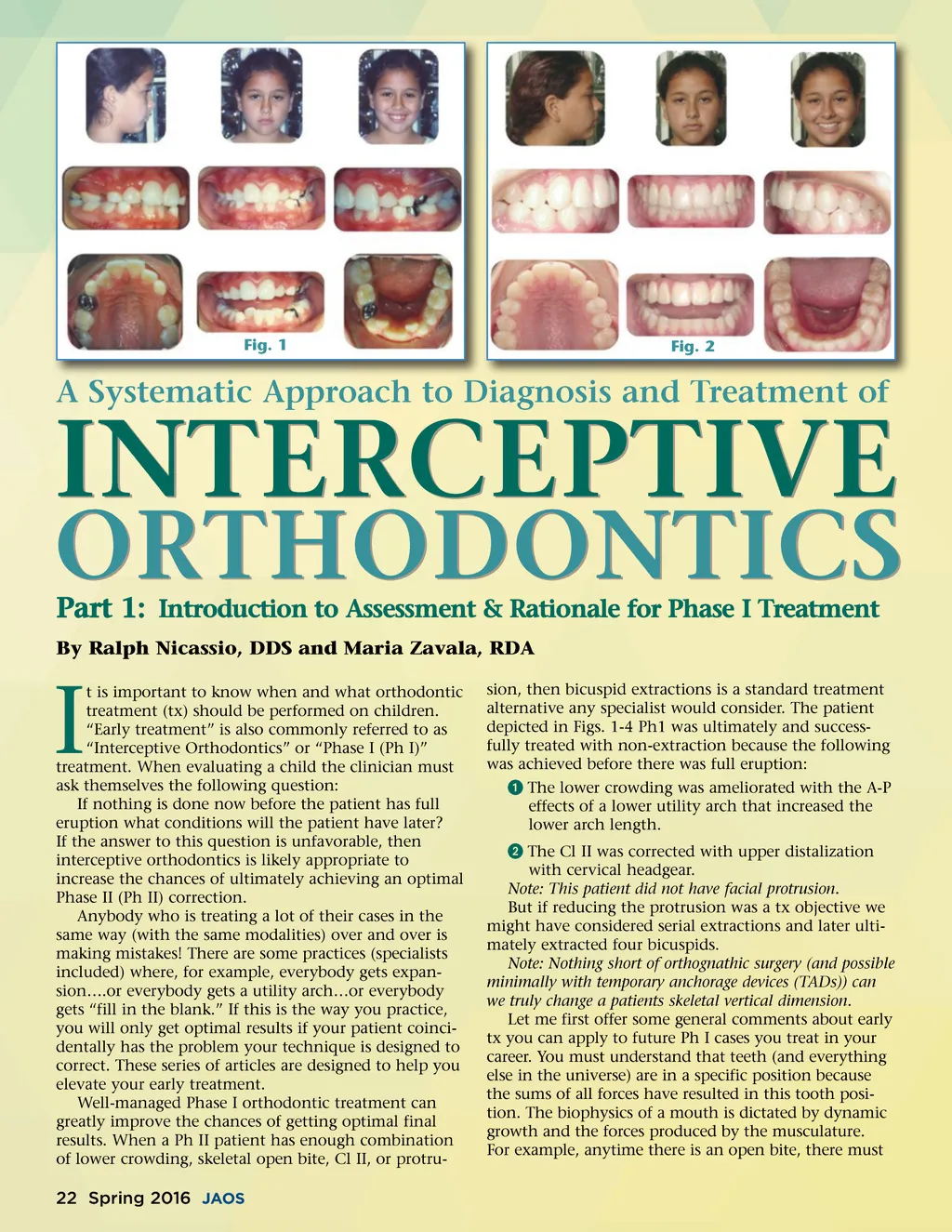
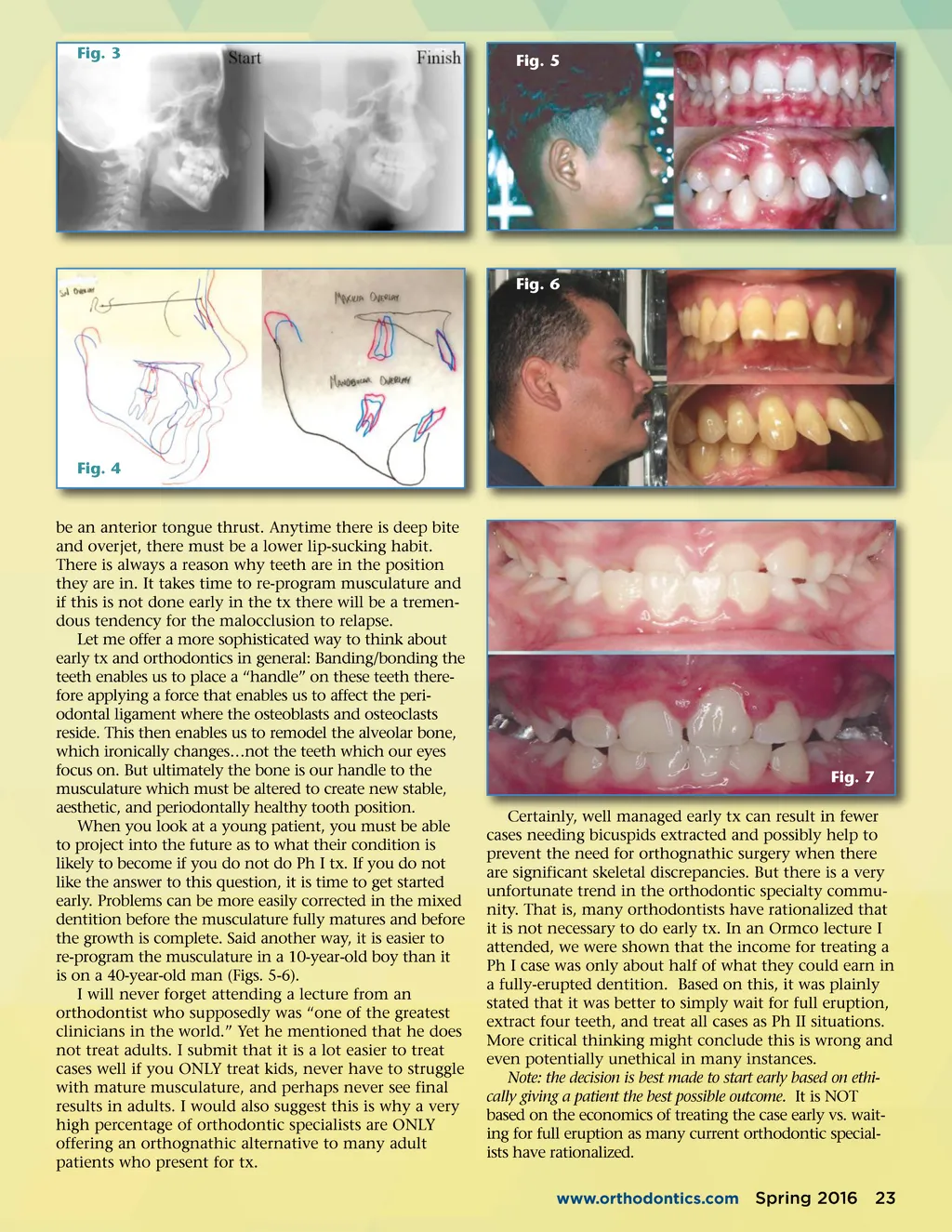
Fig. 3 Fig. 5 Fig. 6 Fig. 4 be an anterior tongue thrust. Anytime there is deep bite and overjet, there must be a lower lip-sucking habit. There is always a reason why teeth are in the position they are in. It takes time to re-program musculature and if this is not done early in the tx there will be a tremen-dous tendency for the malocclusion to relapse. Let me offer a more sophisticated way to think about early tx and orthodontics in general: Banding/bonding the teeth enables us to place a “handle” on these teeth there-fore applying a force that enables us to affect the peri-odontal ligament where the osteoblasts and osteoclasts reside. This then enables us to remodel the alveolar bone, which ironically changes…not the teeth which our eyes focus on. But ultimately the bone is our handle to the musculature which must be altered to create new stable, aesthetic, and periodontally healthy tooth position. When you look at a young patient, you must be able to project into the future as to what their condition is likely to become if you do not do Ph I tx. If you do not like the answer to this question, it is time to get started early. Problems can be more easily corrected in the mixed dentition before the musculature fully matures and before the growth is complete. Said another way, it is easier to re-program the musculature in a 10-year-old boy than it is on a 40-year-old man (Figs. 5-6). I will never forget attending a lecture from an orthodontist who supposedly was “one of the greatest clinicians in the world.” Yet he mentioned that he does not treat adults. I submit that it is a lot easier to treat cases well if you ONLY treat kids, never have to struggle with mature musculature, and perhaps never see final results in adults. I would also suggest this is why a very high percentage of orthodontic specialists are ONLY offering an orthognathic alternative to many adult patients who present for tx. Fig. 7 Certainly, well managed early tx can result in fewer cases needing bicuspids extracted and possibly help to prevent the need for orthognathic surgery when there are significant skeletal discrepancies. But there is a very unfortunate trend in the orthodontic specialty commu-nity. That is, many orthodontists have rationalized that it is not necessary to do early tx. In an Ormco lecture I attended, we were shown that the income for treating a Ph I case was only about half of what they could earn in a fully-erupted dentition. Based on this, it was plainly stated that it was better to simply wait for full eruption, extract four teeth, and treat all cases as Ph II situations. More critical thinking might conclude this is wrong and even potentially unethical in many instances. Note: the decision is best made to start early based on ethi-cally giving a patient the best possible outcome. It is NOT based on the economics of treating the case early vs. wait-ing for full eruption as many current orthodontic special-ists have rationalized. www.orthodontics.com Spring 2016 23
Journal of the American Orthodontic Society Spring 2016: Page 23