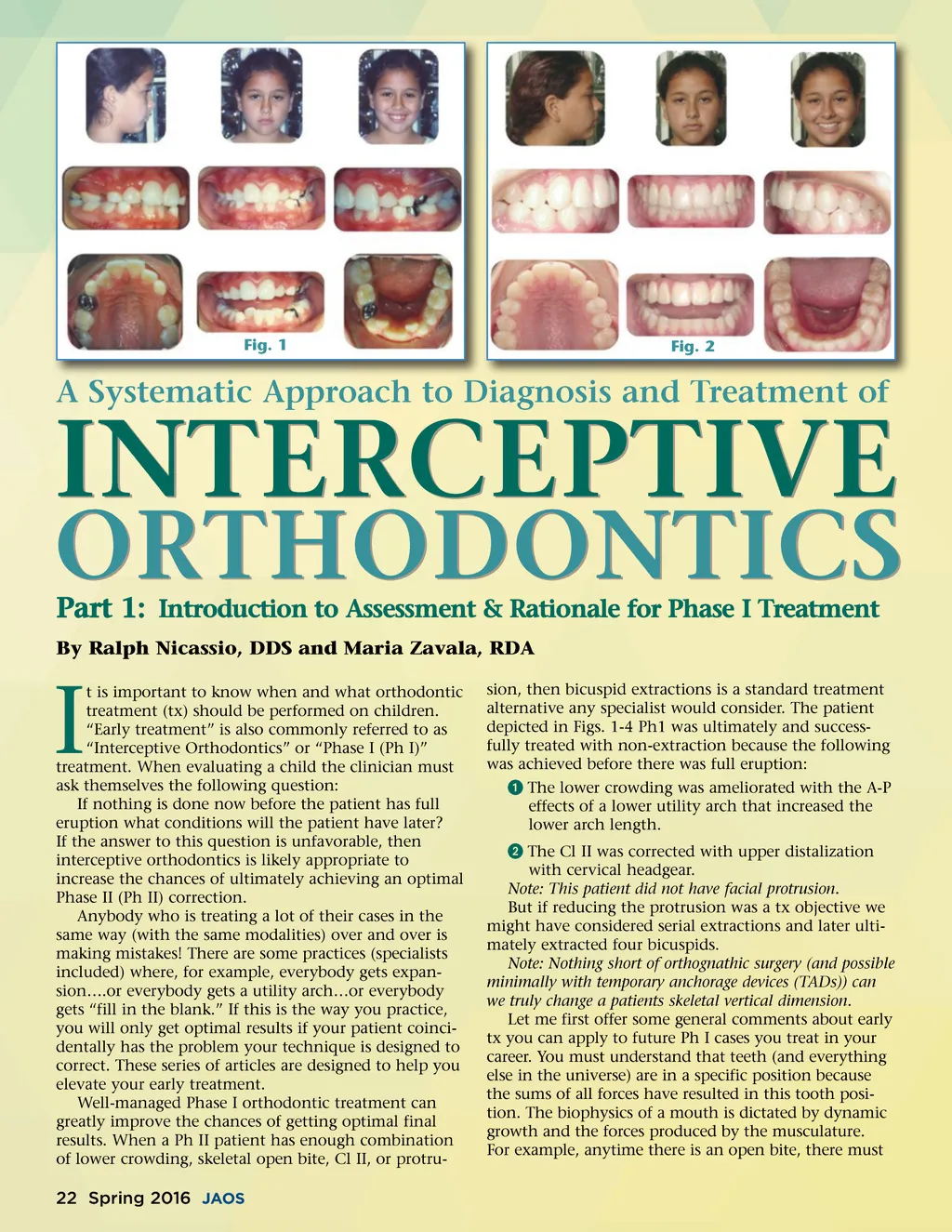
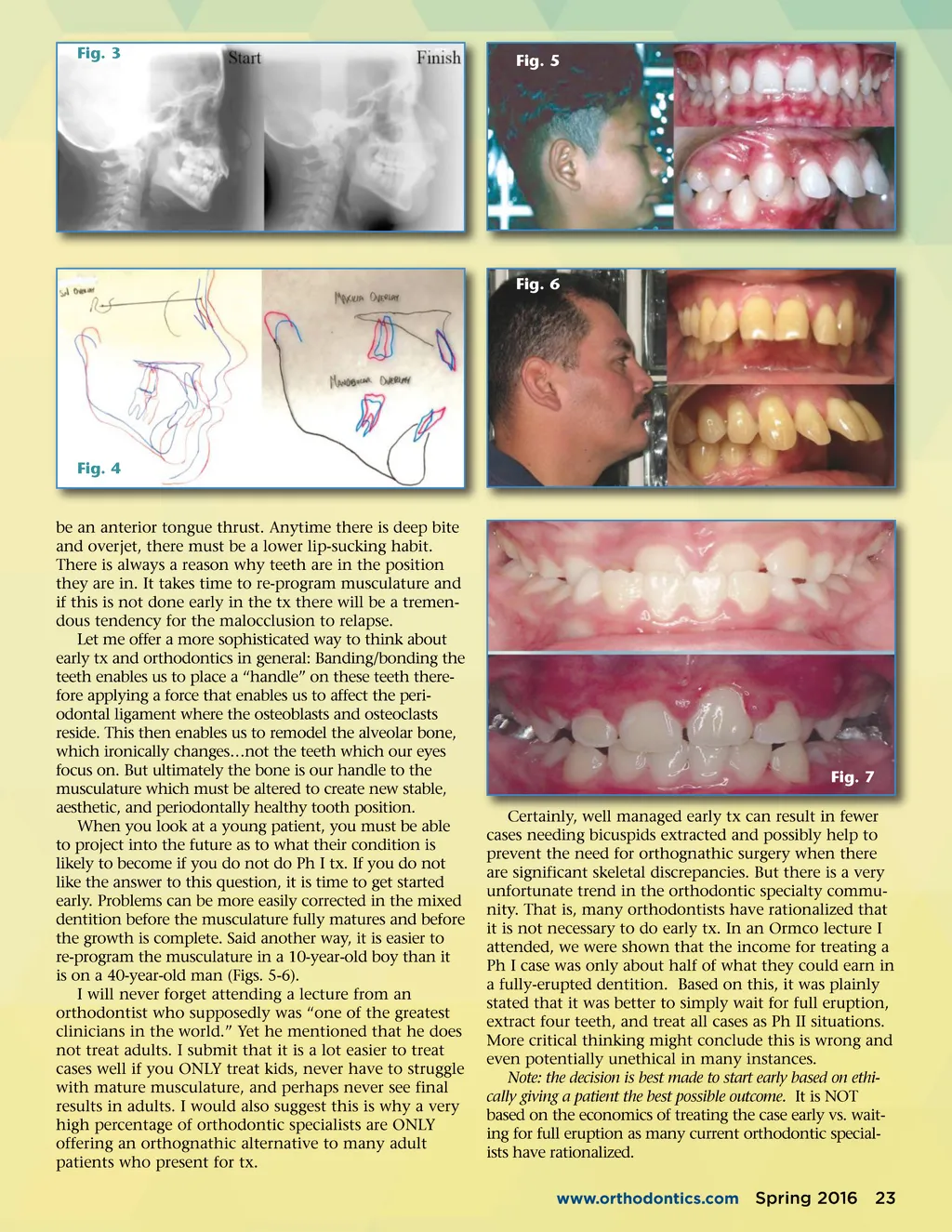
Fig. 1 Fig. 2 A Systematic Approach to Diagnosis and Treatment of INTERCEPTIVE Part 1: Introduction to Assessment & Rationale for Phase I Treatment By Ralph Nicassio, DDS and Maria Zavala, RDA ORTHODONTICS I t is important to know when and what orthodontic treatment (tx) should be performed on children. “Early treatment” is also commonly referred to as “Interceptive Orthodontics” or “Phase I (Ph I)” treatment. When evaluating a child the clinician must ask themselves the following question: If nothing is done now before the patient has full eruption what conditions will the patient have later? If the answer to this question is unfavorable, then interceptive orthodontics is likely appropriate to increase the chances of ultimately achieving an optimal Phase II (Ph II) correction. Anybody who is treating a lot of their cases in the same way (with the same modalities) over and over is making mistakes! There are some practices (specialists included) where, for example, everybody gets expan-sion….or everybody gets a utility arch…or everybody gets “fill in the blank.” If this is the way you practice, you will only get optimal results if your patient coinci-dentally has the problem your technique is designed to correct. These series of articles are designed to help you elevate your early treatment. Well-managed Phase I orthodontic treatment can greatly improve the chances of getting optimal final results. When a Ph II patient has enough combination of lower crowding, skeletal open bite, Cl II, or protru-sion, then bicuspid extractions is a standard treatment alternative any specialist would consider. The patient depicted in Figs. 1-4 Ph1 was ultimately and success-fully treated with non-extraction because the following was achieved before there was full eruption: ᕡ The lower crowding was ameliorated with the A-P effects of a lower utility arch that increased the lower arch length. ᕢ The Cl II was corrected with upper distalization with cervical headgear. Note: This patient did not have facial protrusion. But if reducing the protrusion was a tx objective we might have considered serial extractions and later ulti-mately extracted four bicuspids. Note: Nothing short of orthognathic surgery (and possible minimally with temporary anchorage devices (TADs)) can we truly change a patients skeletal vertical dimension. Let me first offer some general comments about early tx you can apply to future Ph I cases you treat in your career. You must understand that teeth (and everything else in the universe) are in a specific position because the sums of all forces have resulted in this tooth posi-tion. The biophysics of a mouth is dictated by dynamic growth and the forces produced by the musculature. For example, anytime there is an open bite, there must 22 Spring 2016 JAOS
Journal of the American Orthodontic Society Spring 2016: Page 22