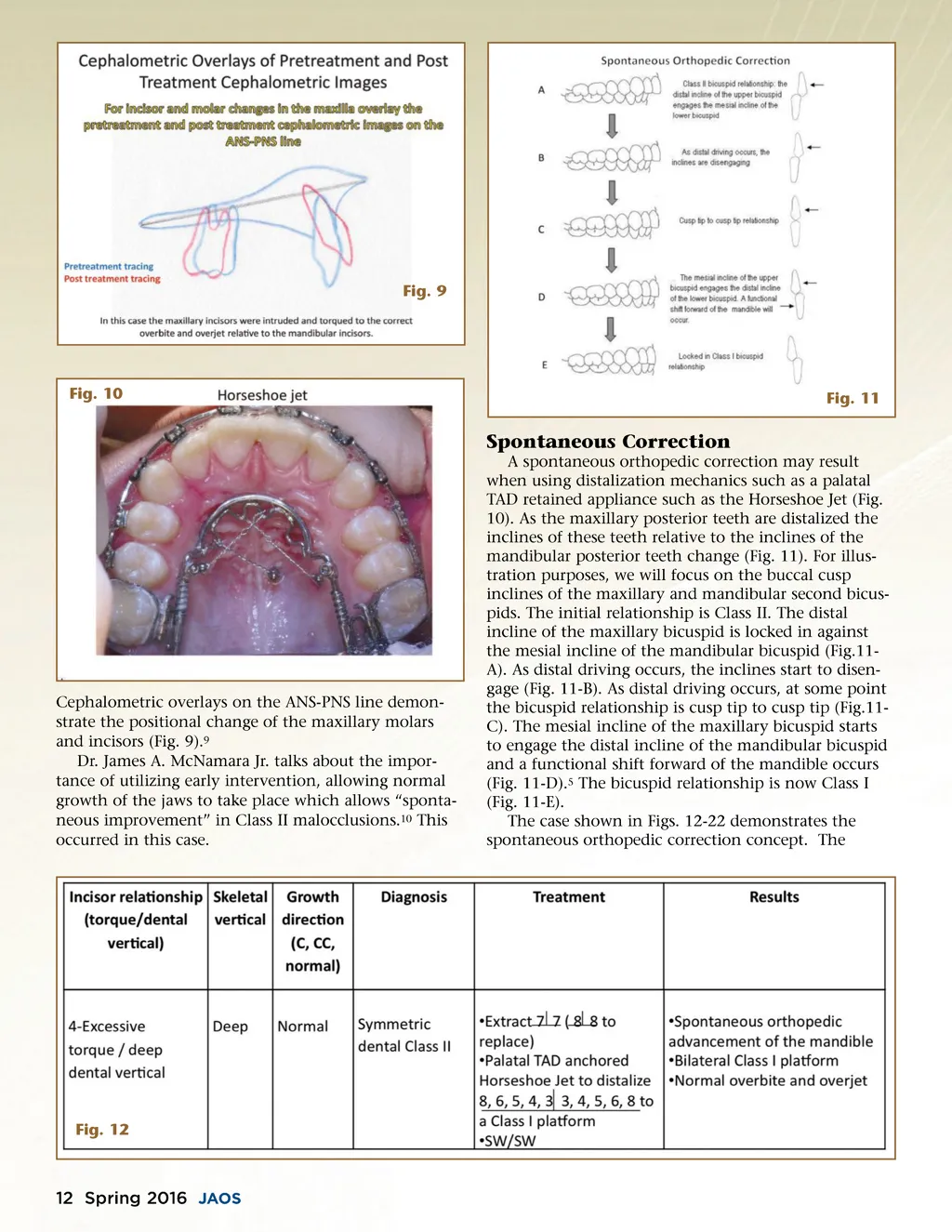
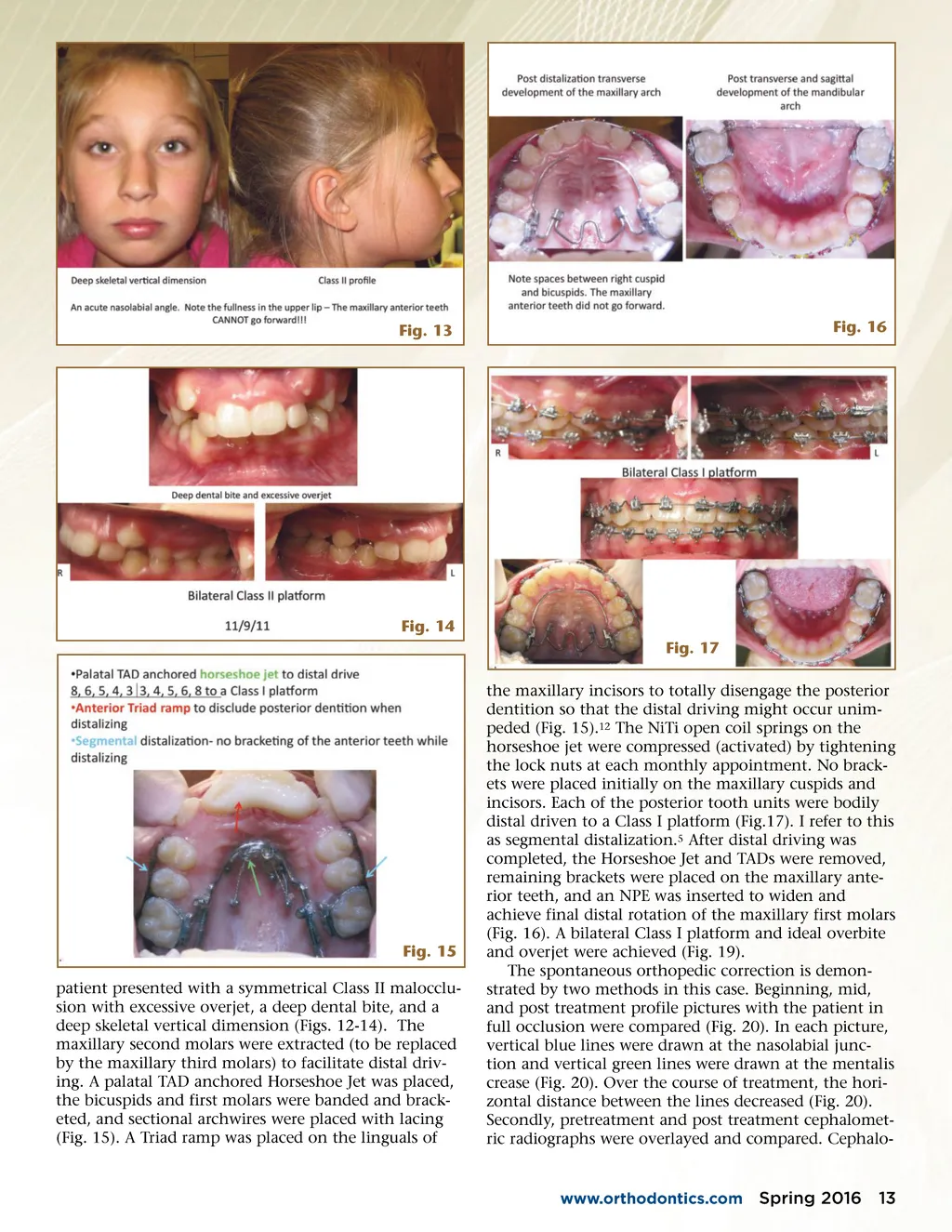
Fig. 13 Fig. 16 Fig. 14 Fig. 17 the maxillary incisors to totally disengage the posterior dentition so that the distal driving might occur unim-peded (Fig. 15). 12 The NiTi open coil springs on the horseshoe jet were compressed (activated) by tightening the lock nuts at each monthly appointment. No brack-ets were placed initially on the maxillary cuspids and incisors. Each of the posterior tooth units were bodily distal driven to a Class I platform (Fig.17). I refer to this as segmental distalization. 5 After distal driving was completed, the Horseshoe Jet and TADs were removed, remaining brackets were placed on the maxillary ante-rior teeth, and an NPE was inserted to widen and achieve final distal rotation of the maxillary first molars (Fig. 16). A bilateral Class I platform and ideal overbite and overjet were achieved (Fig. 19). The spontaneous orthopedic correction is demon-strated by two methods in this case. Beginning, mid, and post treatment profile pictures with the patient in full occlusion were compared (Fig. 20). In each picture, vertical blue lines were drawn at the nasolabial junc-tion and vertical green lines were drawn at the mentalis crease (Fig. 20). Over the course of treatment, the hori-zontal distance between the lines decreased (Fig. 20). Secondly, pretreatment and post treatment cephalomet-ric radiographs were overlayed and compared. Cephalo-Fig. 15 patient presented with a symmetrical Class II malocclu-sion with excessive overjet, a deep dental bite, and a deep skeletal vertical dimension (Figs. 12-14). The maxillary second molars were extracted (to be replaced by the maxillary third molars) to facilitate distal driv-ing. A palatal TAD anchored Horseshoe Jet was placed, the bicuspids and first molars were banded and brack-eted, and sectional archwires were placed with lacing (Fig. 15). A Triad ramp was placed on the linguals of www.orthodontics.com Spring 2016 13
Journal of the American Orthodontic Society Spring 2016: Page 13