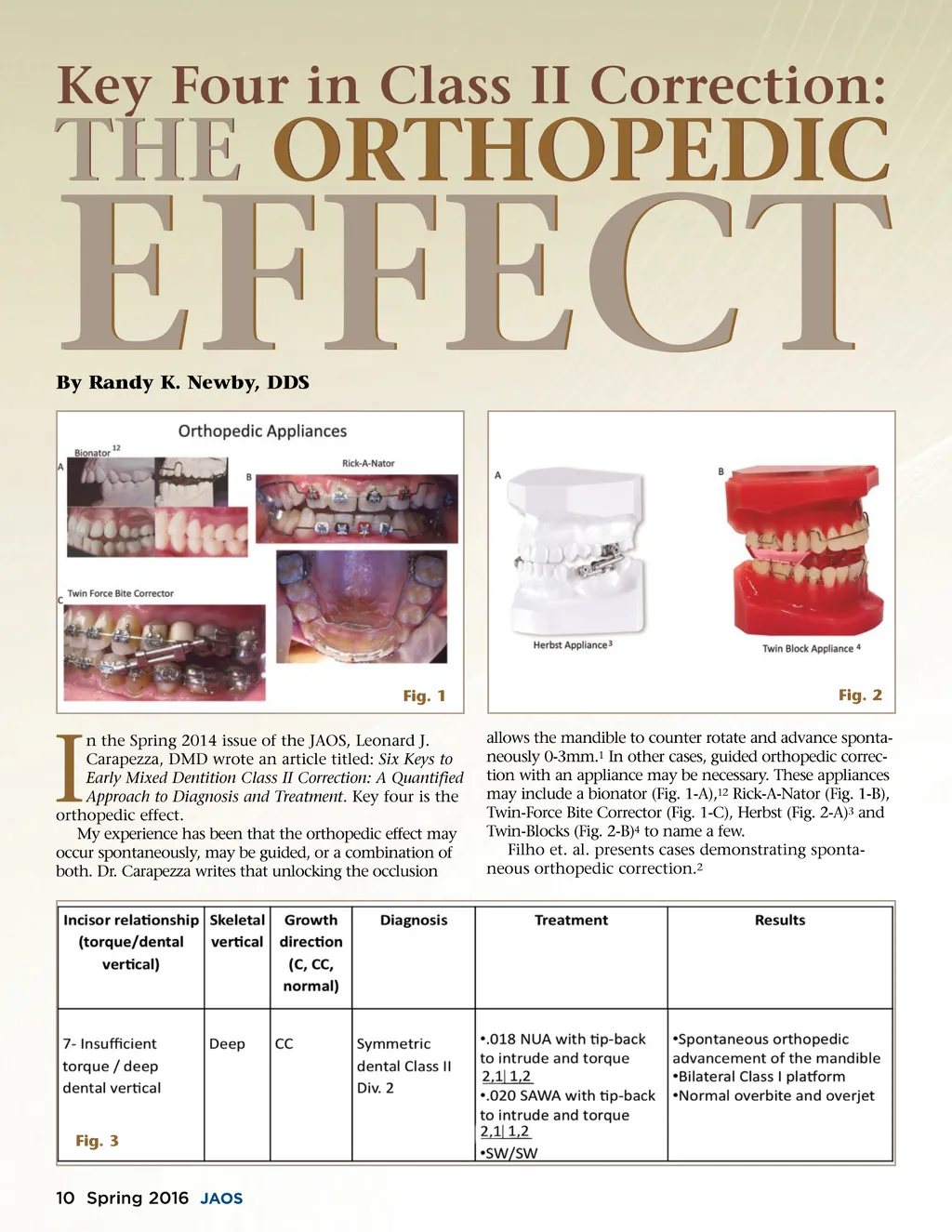
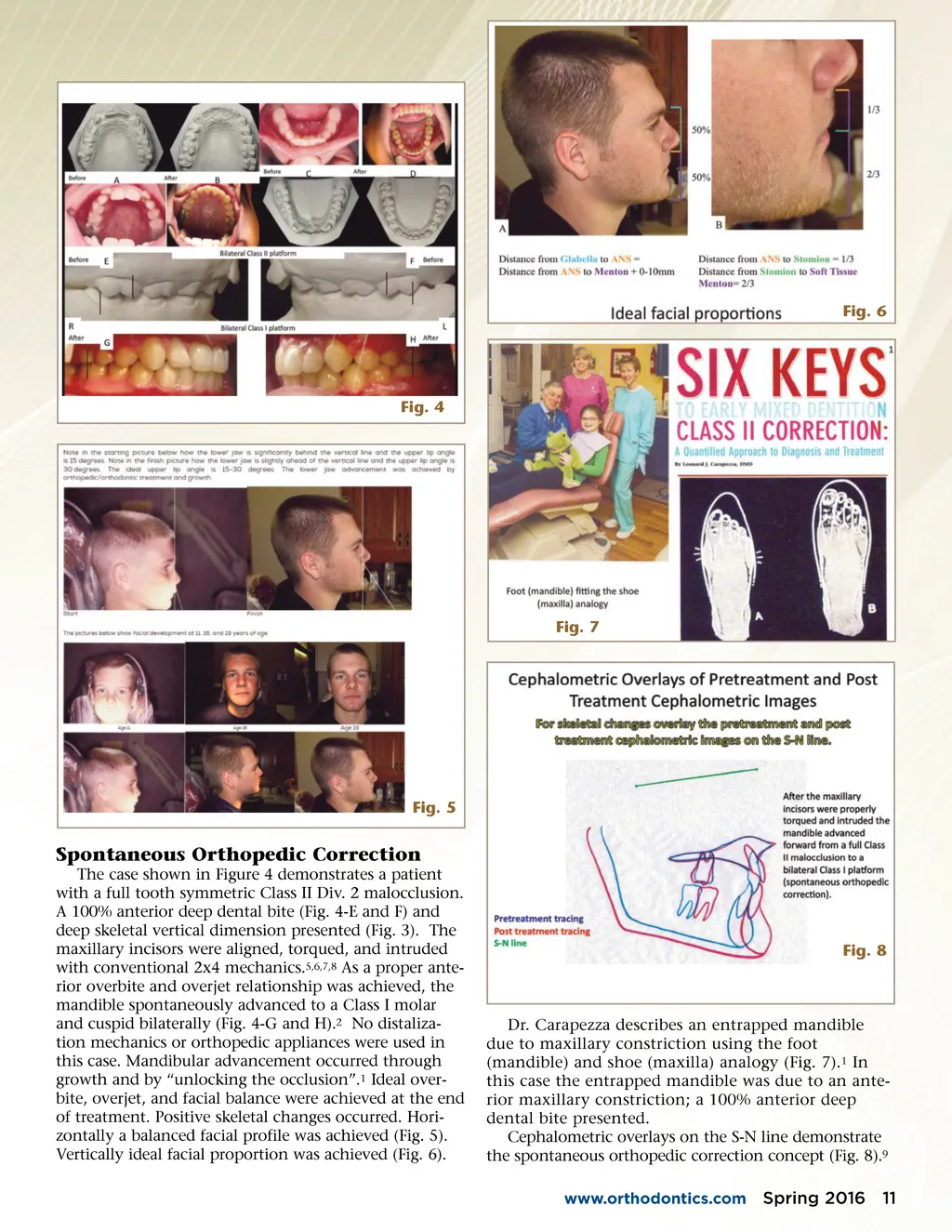
Fig. 6 Fig. 4 Fig. 7 Fig. 5 Spontaneous Orthopedic Correction The case shown in Figure 4 demonstrates a patient with a full tooth symmetric Class II Div. 2 malocclusion. A 100% anterior deep dental bite (Fig. 4-E and F) and deep skeletal vertical dimension presented (Fig. 3). The maxillary incisors were aligned, torqued, and intruded with conventional 2x4 mechanics. 5,6,7,8 As a proper ante-rior overbite and overjet relationship was achieved, the mandible spontaneously advanced to a Class I molar and cuspid bilaterally (Fig. 4-G and H). 2 No distaliza-tion mechanics or orthopedic appliances were used in this case. Mandibular advancement occurred through growth and by “unlocking the occlusion”. 1 Ideal over-bite, overjet, and facial balance were achieved at the end of treatment. Positive skeletal changes occurred. Hori-zontally a balanced facial profile was achieved (Fig. 5). Vertically ideal facial proportion was achieved (Fig. 6). Fig. 8 Dr. Carapezza describes an entrapped mandible due to maxillary constriction using the foot (mandible) and shoe (maxilla) analogy (Fig. 7). 1 In this case the entrapped mandible was due to an ante-rior maxillary constriction; a 100% anterior deep dental bite presented. Cephalometric overlays on the S-N line demonstrate the spontaneous orthopedic correction concept (Fig. 8). 9 www.orthodontics.com Spring 2016 11
Journal of the American Orthodontic Society Spring 2016: Page 11