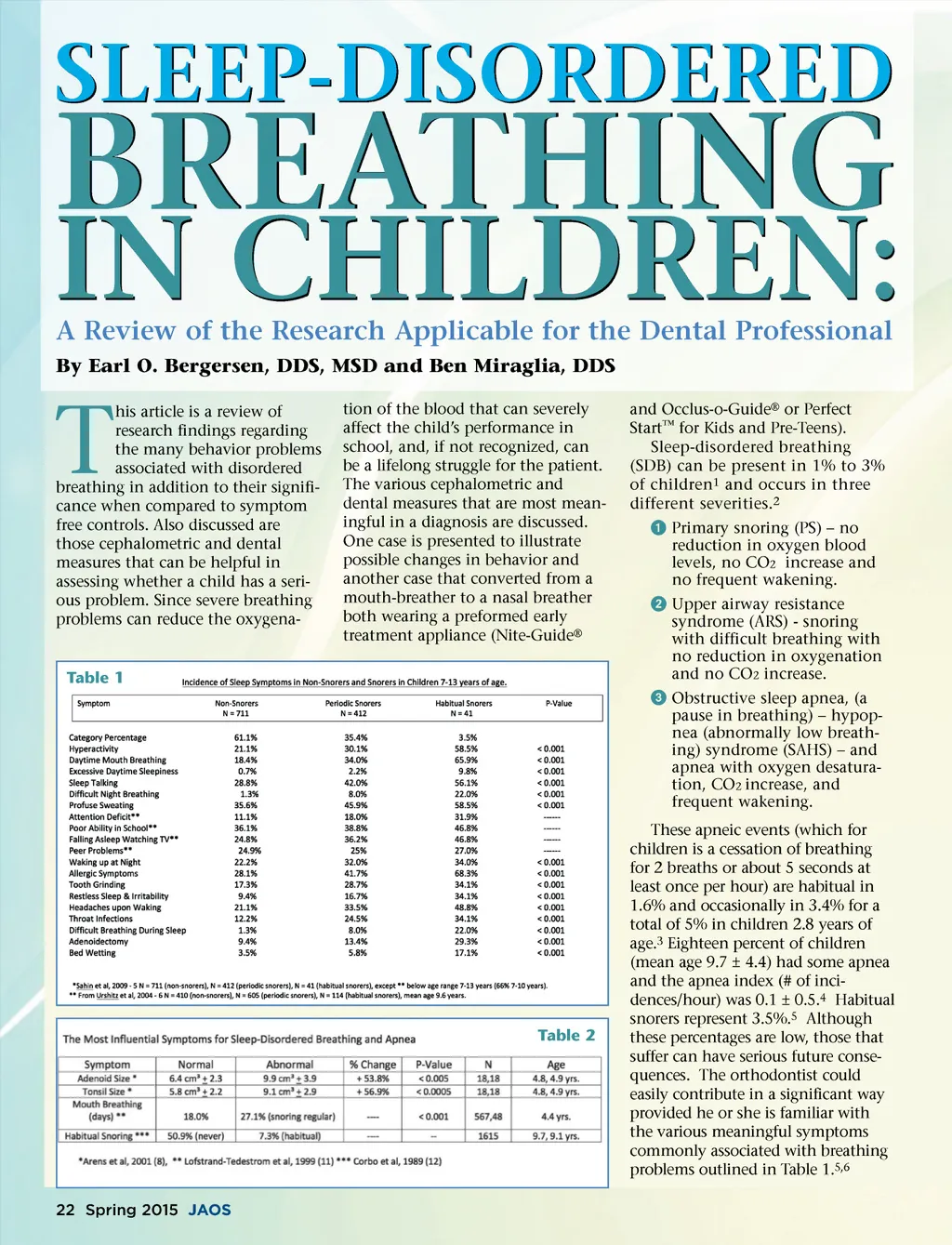
Table 2 presents the four most frequent symptoms involving sleep-disordered breathing (SBD). The most frequent is swollen adenoids with enlarged tonsils 7 close behind. An accurate estimate of their size can be made with an MRI, 8 however a simple oral examination can indi-cate if the tonsils are swollen and adenoid size can be seen on a lateral cephalometric radiograph. If enlargement is suspected, the patient can be referred to a special-ist. Swollen tonsils can slightly displace towards the pharynx when the patient lies down and can cause pharyngeal obstruction in a supine position when they seem more normal when the patient is vertical. 9 Adenoids and tonsils are at their peak size between 3 and 6 years of age 10 and an adenotonsilec-tomy is often all that is needed to solve a serious breathing problem in a young child. Two other important diagnostic symptoms in Table 2 are daytime and nighttime open-mouth breath-ing, 11 and habitual snoring. 12 The presence of these two characteristics should be a strong indication for a parent questionaire 13 and if apnea is suspected, a home night study and a lateral cephalometric radiograph would be recommended. A home night study is a reliable diagnostic aid to determine the presence of sleep apnea, hypopnea, and oxygen desaturation. 14 Any indication for sleep apnea should be referred for an overnight study called a polysomnograph. Many of the behavior problems in Table 1 do not improve with an increase in age, 15 however, there are three behavioral problems that seem to be very important, namely inattention or attention deficit, hyperactivity and daytime sleepi-ness. 13 When these symptoms are present, a correct diagnosis becomes more assured. Two studies were used to prepare Table 1. 5,6 While other studies confirm such symp-toms. 15-23 Helpful guidelines have been established as to a recom-mended protocol in children that can be helpful in a diagnosis. 24 A rather typical example of a patient who had several of the Fig. 1 symptoms listed in Table 1, was an habitual-snoring male patient, 6½ years old, in the second grade, with symptoms such as hyperactivity, attention deficit, mild aggressive-ness to peers, limited school success, periodic bed wetting, sleep walking, and excessive movement during sleep, often sitting up in bed without waking. The patient was immediately given an Eruption Guidance Appliance ® called Nite-Guide ® *, or Perfect Start ™ for Kids. This appliance serves as a template to properly guide the permanent upper and lower incisors into the mouth. As these teeth erupt with-out rotations, and without displace-ment, they force the arch (upper and lower) to enlarge to properly accommodate the larger permanent incisors. Once the lower central incisors were completely erupted, an Occlus-o-Guide ® , or Perfect Start ™ for Kids was inserted, which allowed further arch enlargement to occur. The patient’s upper arch increased a total of 6 mm. while the lower increased 4 mm. At the same time, the posterior maxillary segment enlarges by 3.5 mm. at the level of the first permanent molars. The maxillary left central erupted lingually and was about 1 mm. crowded (Fig. 1). This enlargement occurs gradually as the maxillary and mandibular incisors erupt, and Fig. 2 www.orthodontics.com Spring 2015 23
Journal of the American Orthodontic Society Spring 2015: Page 23