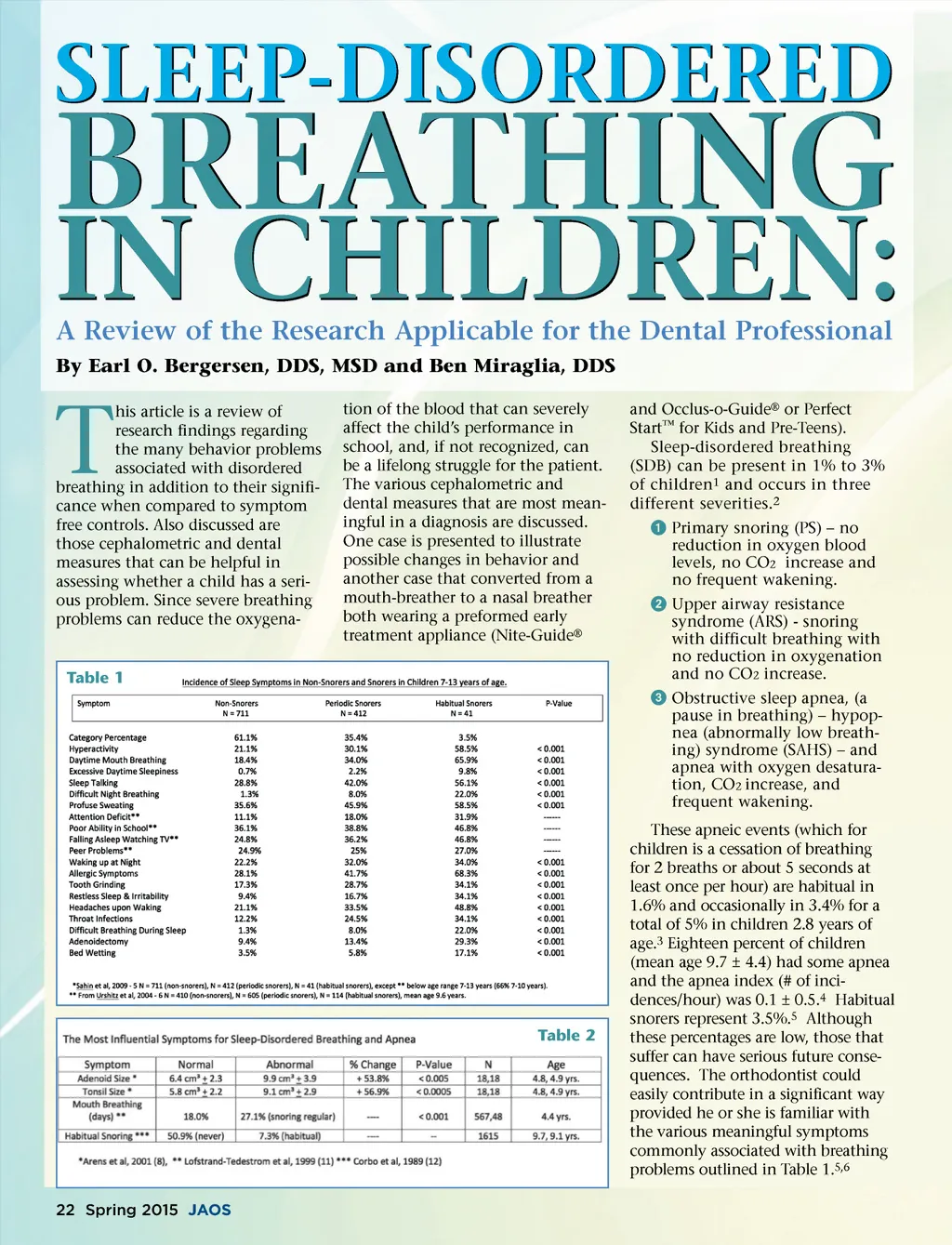
BREATHING A Review of the Research Applicable for the Dental Professional tion of the blood that can severely affect the child’s performance in school, and, if not recognized, can be a lifelong struggle for the patient. The various cephalometric and dental measures that are most mean-ingful in a diagnosis are discussed. One case is presented to illustrate possible changes in behavior and another case that converted from a mouth-breather to a nasal breather both wearing a preformed early treatment appliance (Nite-Guide ® and Occlus-o-Guide ® or Perfect Start ™ for Kids and Pre-Teens). Sleep-disordered breathing (SDB) can be present in 1% to 3% of children 1 and occurs in three different severities. 2 ᕡ Primary snoring (PS) – no reduction in oxygen blood levels, no CO 2 increase and no frequent wakening. ᕢ Upper airway resistance syndrome (ARS) -snoring with difficult breathing with no reduction in oxygenation and no CO 2 increase. ᕣ Obstructive sleep apnea, (a pause in breathing) – hypop-nea (abnormally low breath-ing) syndrome (SAHS) – and apnea with oxygen desatura-tion, CO 2 increase, and frequent wakening. These apneic events (which for children is a cessation of breathing for 2 breaths or about 5 seconds at least once per hour) are habitual in 1.6% and occasionally in 3.4% for a total of 5% in children 2.8 years of age. 3 Eighteen percent of children (mean age 9.7 ± 4.4) had some apnea and the apnea index (# of inci-dences/hour) was 0.1 ± 0.5. 4 Habitual snorers represent 3.5%. 5 Although these percentages are low, those that suffer can have serious future conse-quences. The orthodontist could easily contribute in a significant way provided he or she is familiar with the various meaningful symptoms commonly associated with breathing problems outlined in Table 1. 5,6 SLEEP-DISORDERED IN CHILDREN: By Earl O. Bergersen, DDS, MSD and Ben Miraglia, DDS T his article is a review of research findings regarding the many behavior problems associated with disordered breathing in addition to their signifi-cance when compared to symptom free controls. Also discussed are those cephalometric and dental measures that can be helpful in assessing whether a child has a seri-ous problem. Since severe breathing problems can reduce the oxygena-Table 1 Table 2 22 Spring 2015 JAOS
Journal of the American Orthodontic Society Spring 2015: Page 22