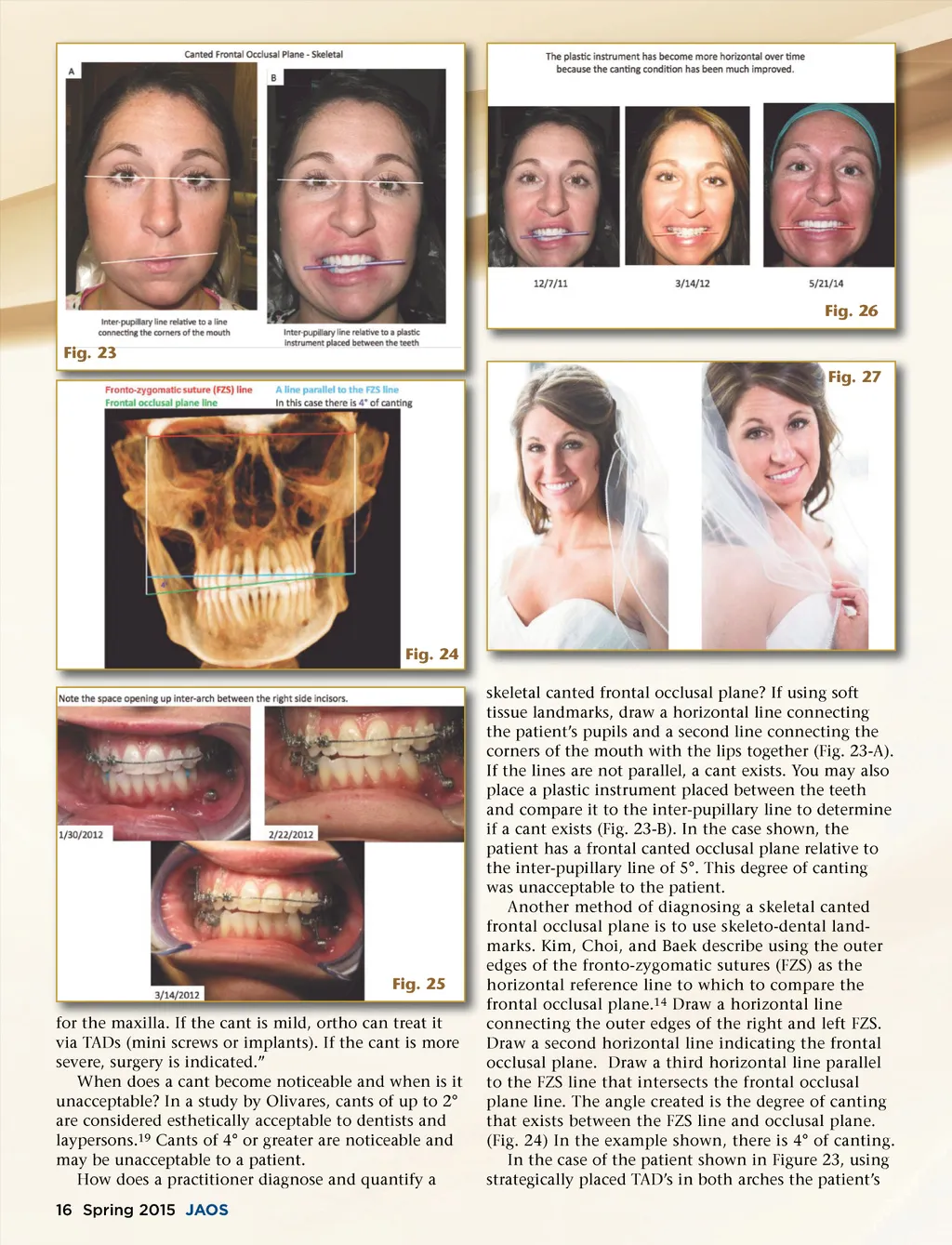
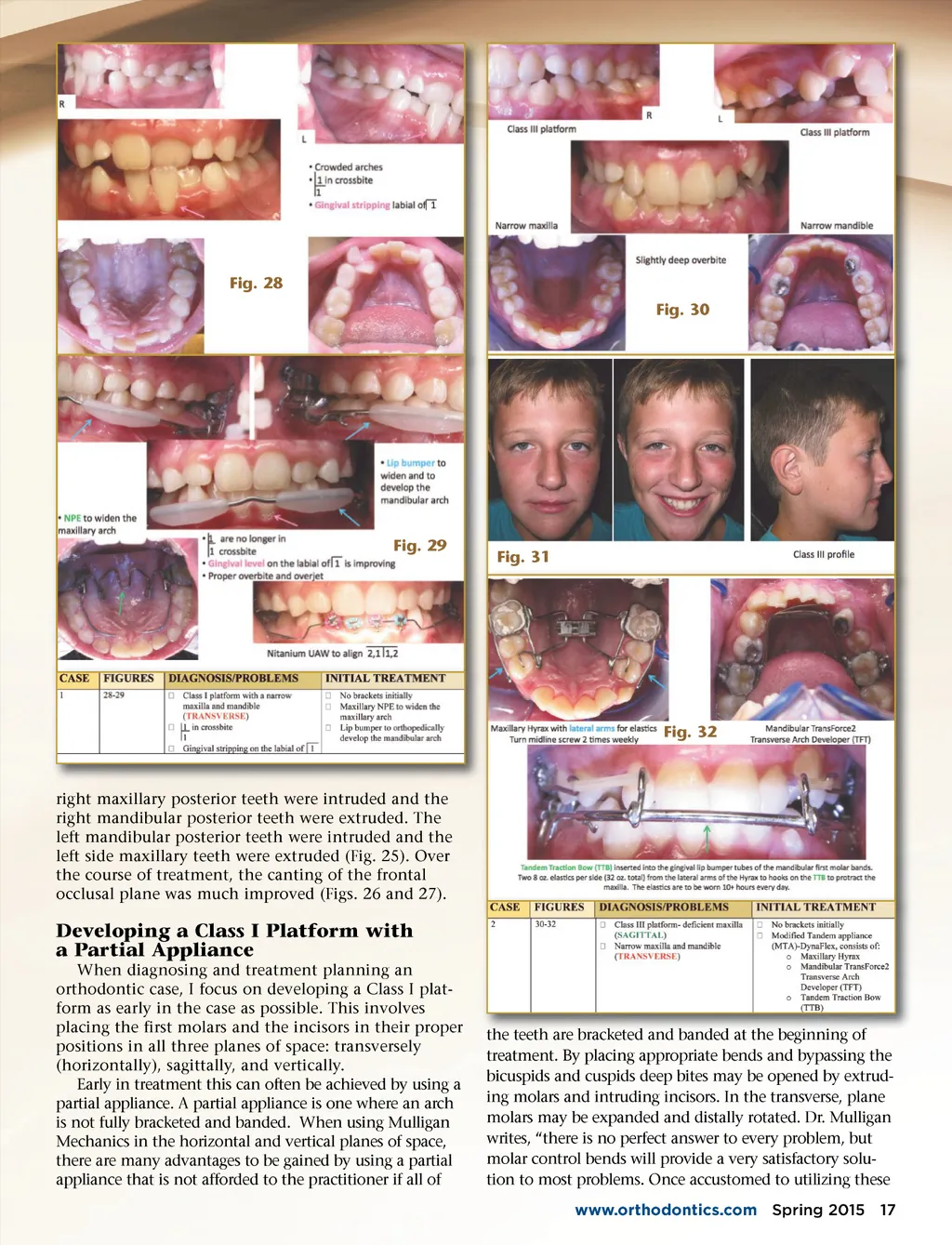
Fig. 26 Fig. 23 Fig. 27 Fig. 24 skeletal canted frontal occlusal plane? If using soft tissue landmarks, draw a horizontal line connecting the patient’s pupils and a second line connecting the corners of the mouth with the lips together (Fig. 23-A). If the lines are not parallel, a cant exists. You may also place a plastic instrument placed between the teeth and compare it to the inter-pupillary line to determine if a cant exists (Fig. 23-B). In the case shown, the patient has a frontal canted occlusal plane relative to the inter-pupillary line of 5°. This degree of canting was unacceptable to the patient. Another method of diagnosing a skeletal canted frontal occlusal plane is to use skeleto-dental land-marks. Kim, Choi, and Baek describe using the outer edges of the fronto-zygomatic sutures (FZS) as the horizontal reference line to which to compare the frontal occlusal plane. 14 Draw a horizontal line connecting the outer edges of the right and left FZS. Draw a second horizontal line indicating the frontal occlusal plane. Draw a third horizontal line parallel to the FZS line that intersects the frontal occlusal plane line. The angle created is the degree of canting that exists between the FZS line and occlusal plane. (Fig. 24) In the example shown, there is 4° of canting. In the case of the patient shown in Figure 23, using strategically placed TAD’s in both arches the patient’s Fig. 25 maxilla. If the cant is mild mild, ortho can treat it for the maxilla via TADs (mini screws or implants). If the cant is more severe, surgery is indicated.” When does a cant become noticeable and when is it unacceptable? In a study by Olivares, cants of up to 2° are considered esthetically acceptable to dentists and laypersons. 19 Cants of 4° or greater are noticeable and may be unacceptable to a patient. How does a practitioner diagnose and quantify a 16 Spring 2015 JAOS
Journal of the American Orthodontic Society Spring 2015: Page 16