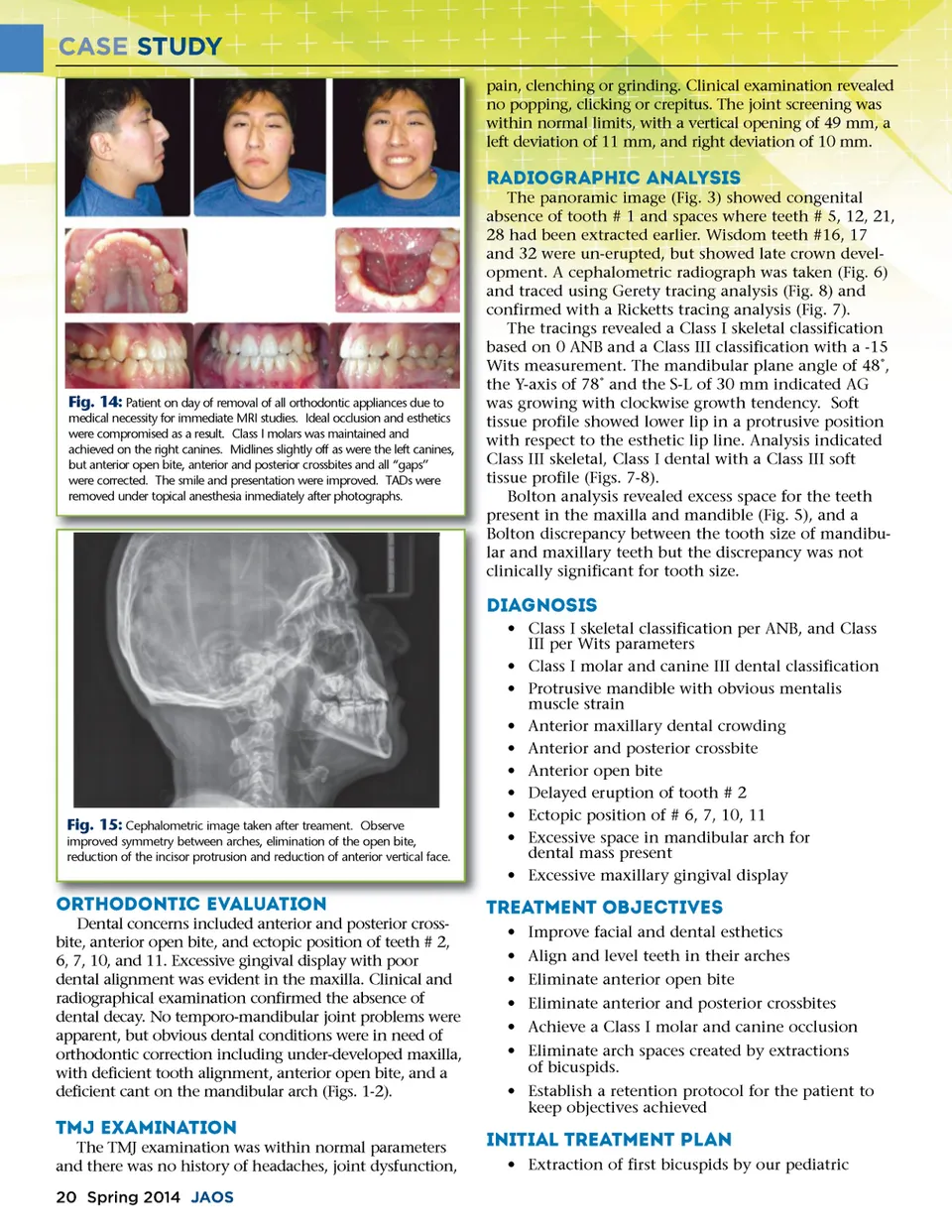
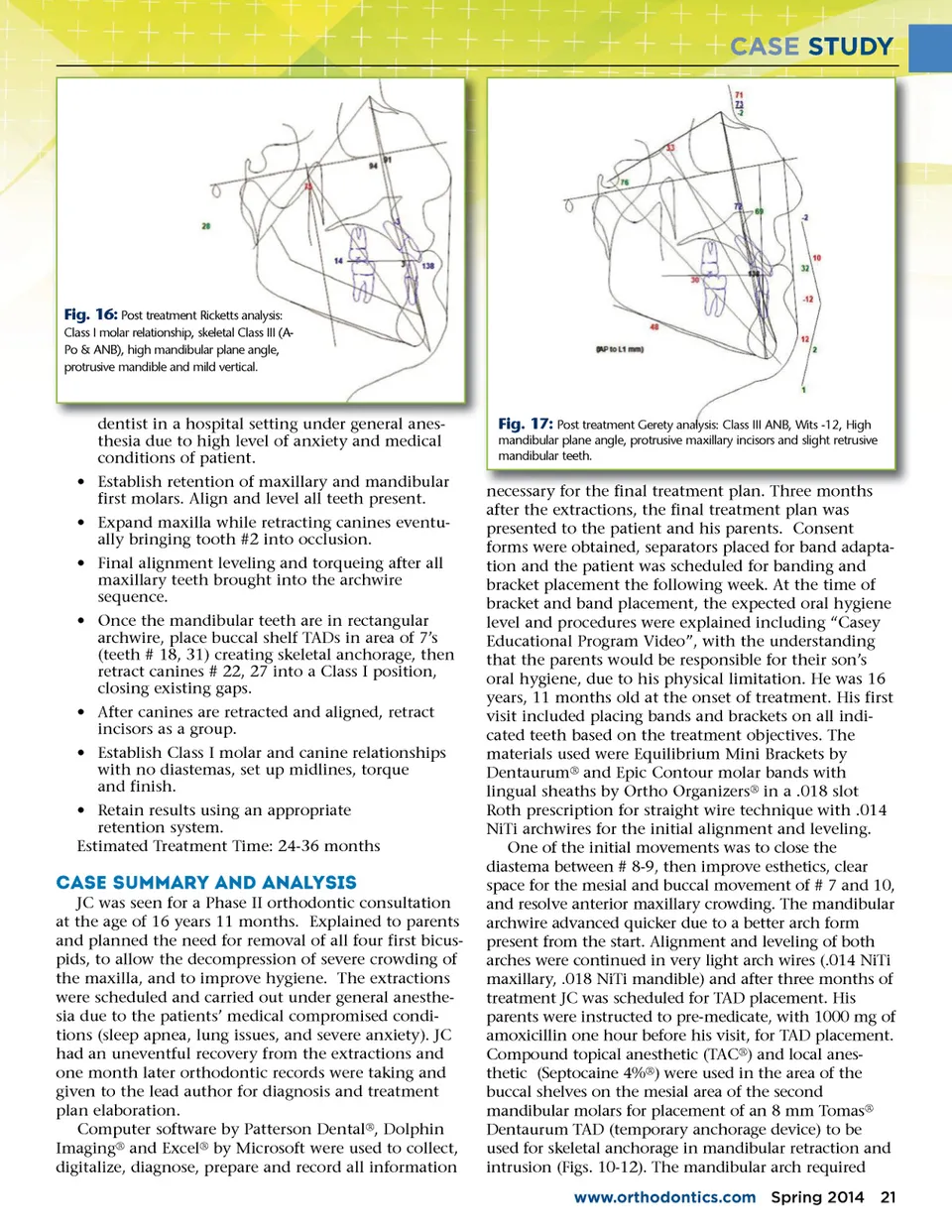
CASE STUDY Fig. 16: Post treatment Ricketts analysis: Class I molar relationship, skeletal Class III (A-Po & ANB), high mandibular plane angle, protrusive mandible and mild vertical. dentist in a hospital setting under general anes anes-thesia due to high level of anxiety and medical conditions of patient. • Establish retention of maxillary and mandibular first molars. Align and level all teeth present. • Expand maxilla while retracting canines eventu-ally bringing tooth #2 into occlusion. • Final alignment leveling and torqueing after all maxillary teeth brought into the archwire sequence. • Once the mandibular teeth are in rectangular archwire, place buccal shelf TADs in area of 7’s (teeth # 18, 31) creating skeletal anchorage, then retract canines # 22, 27 into a Class I position, closing existing gaps. • After canines are retracted and aligned, retract incisors as a group. • Establish Class I molar and canine relationships with no diastemas, set up midlines, torque and finish. • Retain results using an appropriate retention system. Estimated Treatment Time: 24-36 months Fig. 17: Post treatment Gerety analysis: Class III ANB, Wits -12, High mandibular plane angle, protrusive maxillary incisors and slight retrusive mandibular teeth. plan. Three months necessary for the final treatment plan after the extractions, the final treatment plan was presented to the patient and his parents. Consent forms were obtained, separators placed for band adapta-tion and the patient was scheduled for banding and bracket placement the following week. At the time of bracket and band placement, the expected oral hygiene level and procedures were explained including “Casey Educational Program Video”, with the understanding that the parents would be responsible for their son’s oral hygiene, due to his physical limitation. He was 16 years, 11 months old at the onset of treatment. His first visit included placing bands and brackets on all indi-cated teeth based on the treatment objectives. The materials used were Equilibrium Mini Brackets by Dentaurum ® and Epic Contour molar bands with lingual sheaths by Ortho Organizers ® in a .018 slot Roth prescription for straight wire technique with .014 NiTi archwires for the initial alignment and leveling. One of the initial movements was to close the diastema between # 8-9, then improve esthetics, clear space for the mesial and buccal movement of # 7 and 10, and resolve anterior maxillary crowding. The mandibular archwire advanced quicker due to a better arch form present from the start. Alignment and leveling of both arches were continued in very light arch wires (.014 NiTi maxillary, .018 NiTi mandible) and after three months of treatment JC was scheduled for TAD placement. His parents were instructed to pre-medicate, with 1000 mg of amoxicillin one hour before his visit, for TAD placement. Compound topical anesthetic (TAC ® ) and local anes-thetic (Septocaine 4% ® ) were used in the area of the buccal shelves on the mesial area of the second mandibular molars for placement of an 8 mm Tomas ® Dentaurum TAD (temporary anchorage device) to be used for skeletal anchorage in mandibular retraction and intrusion (Figs. 10-12). The mandibular arch required www.orthodontics.com Spring 2014 21 Case Summary and Analysis JC was seen for a Phase II orthodontic consultation at the age of 16 years 11 months. Explained to parents and planned the need for removal of all four first bicus-pids, to allow the decompression of severe crowding of the maxilla, and to improve hygiene. The extractions were scheduled and carried out under general anesthe-sia due to the patients’ medical compromised condi-tions (sleep apnea, lung issues, and severe anxiety). JC had an uneventful recovery from the extractions and one month later orthodontic records were taking and given to the lead author for diagnosis and treatment plan elaboration. Computer software by Patterson Dental ® , Dolphin Imaging ® and Excel ® by Microsoft were used to collect, digitalize, diagnose, prepare and record all information
Journal of the American Orthodontic Society Spring 2014: Page 21