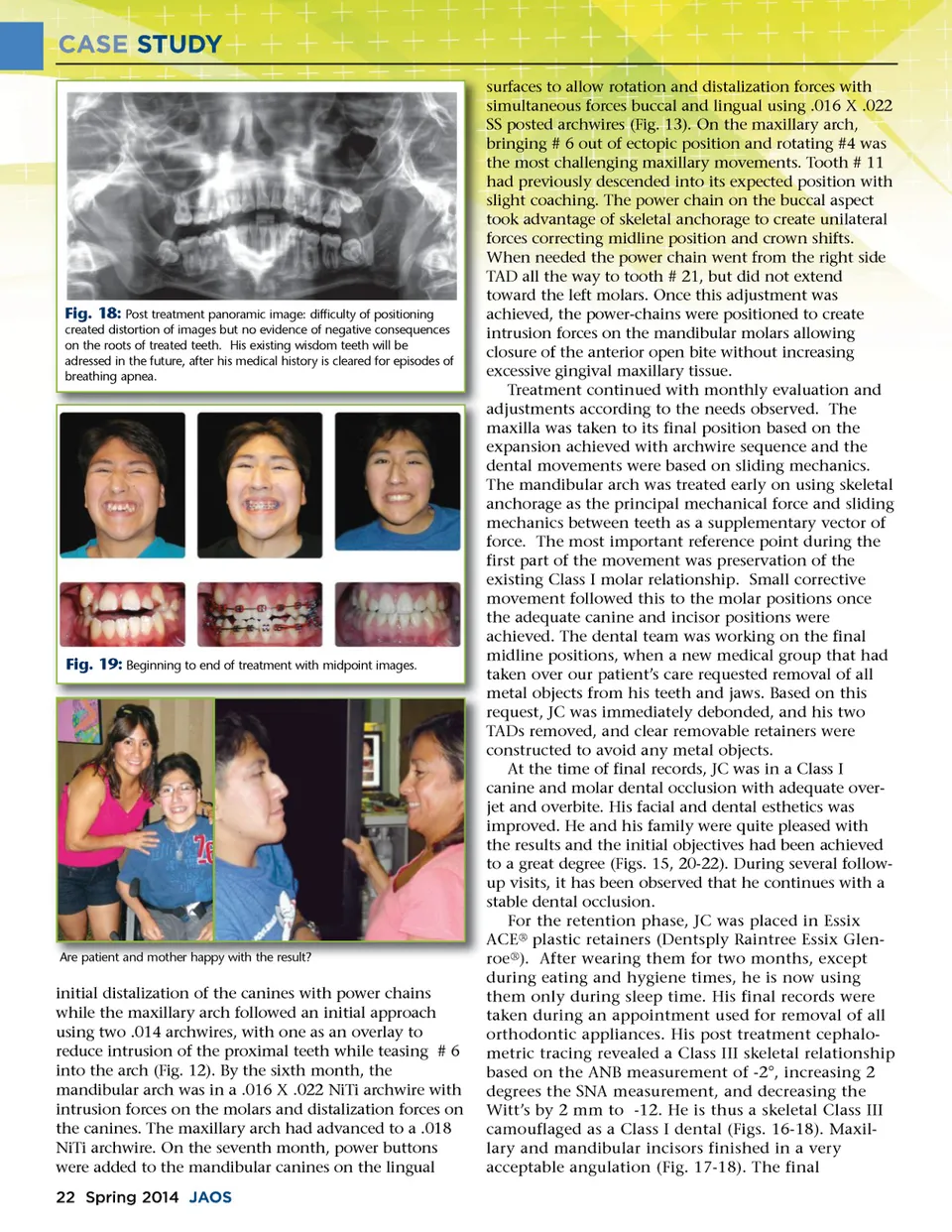
CASE STUDY surfaces to allow rotation and distalization forces with simultaneous forces buccal and lingual using .016 X .022 SS posted archwires (Fig. 13). On the maxillary arch, bringing # 6 out of ectopic position and rotating #4 was the most challenging maxillary movements. Tooth # 11 had previously descended into its expected position with slight coaching. The power chain on the buccal aspect took advantage of skeletal anchorage to create unilateral forces correcting midline position and crown shifts. When needed the power chain went from the right side TAD all the way to tooth # 21, but did not extend toward the left molars. Once this adjustment was achieved, the power-chains were positioned to create intrusion forces on the mandibular molars allowing closure of the anterior open bite without increasing excessive gingival maxillary tissue. Treatment continued with monthly evaluation and adjustments according to the needs observed. The maxilla was taken to its final position based on the expansion achieved with archwire sequence and the dental movements were based on sliding mechanics. The mandibular arch was treated early on using skeletal anchorage as the principal mechanical force and sliding mechanics between teeth as a supplementary vector of force. The most important reference point during the first part of the movement was preservation of the existing Class I molar relationship. Small corrective movement followed this to the molar positions once the adequate canine and incisor positions were achieved. The dental team was working on the final midline positions, when a new medical group that had taken over our patient’s care requested removal of all metal objects from his teeth and jaws. Based on this request, JC was immediately debonded, and his two TADs removed, and clear removable retainers were constructed to avoid any metal objects. At the time of final records, JC was in a Class I canine and molar dental occlusion with adequate over-jet and overbite. His facial and dental esthetics was improved. He and his family were quite pleased with the results and the initial objectives had been achieved to a great degree (Figs. 15, 20-22). During several follow-up visits, it has been observed that he continues with a stable dental occlusion. For the retention phase, JC was placed in Essix ACE ® plastic retainers (Dentsply Raintree Essix Glen-roe ® ). After wearing them for two months, except during eating and hygiene times, he is now using them only during sleep time. His final records were taken during an appointment used for removal of all orthodontic appliances. His post treatment cephalo-metric tracing revealed a Class III skeletal relationship based on the ANB measurement of -2°, increasing 2 degrees the SNA measurement, and decreasing the Witt’s by 2 mm to -12. He is thus a skeletal Class III camouflaged as a Class I dental (Figs. 16-18). Maxil-lary and mandibular incisors finished in a very acceptable angulation (Fig. 17-18). The final Fig. 18: Post treatment panoramic image: difficulty of positioning created distortion of images but no evidence of negative consequences on the roots of treated teeth. His existing wisdom teeth will be adressed in the future, after his medical history is cleared for episodes of breathing apnea. Fig. 19: Beginning to end of treatment with midpoint images. Are patient and mother happy with the result? initial distalization of the canines with power chains while the maxillary arch followed an initial approach using two .014 archwires, with one as an overlay to reduce intrusion of the proximal teeth while teasing # 6 into the arch (Fig. 12). By the sixth month, the mandibular arch was in a .016 X .022 NiTi archwire with intrusion forces on the molars and distalization forces on the canines. The maxillary arch had advanced to a .018 NiTi archwire. On the seventh month, power buttons were added to the mandibular canines on the lingual 22 Spring 2014 JAOS
Journal of the American Orthodontic Society Spring 2014: Page 22