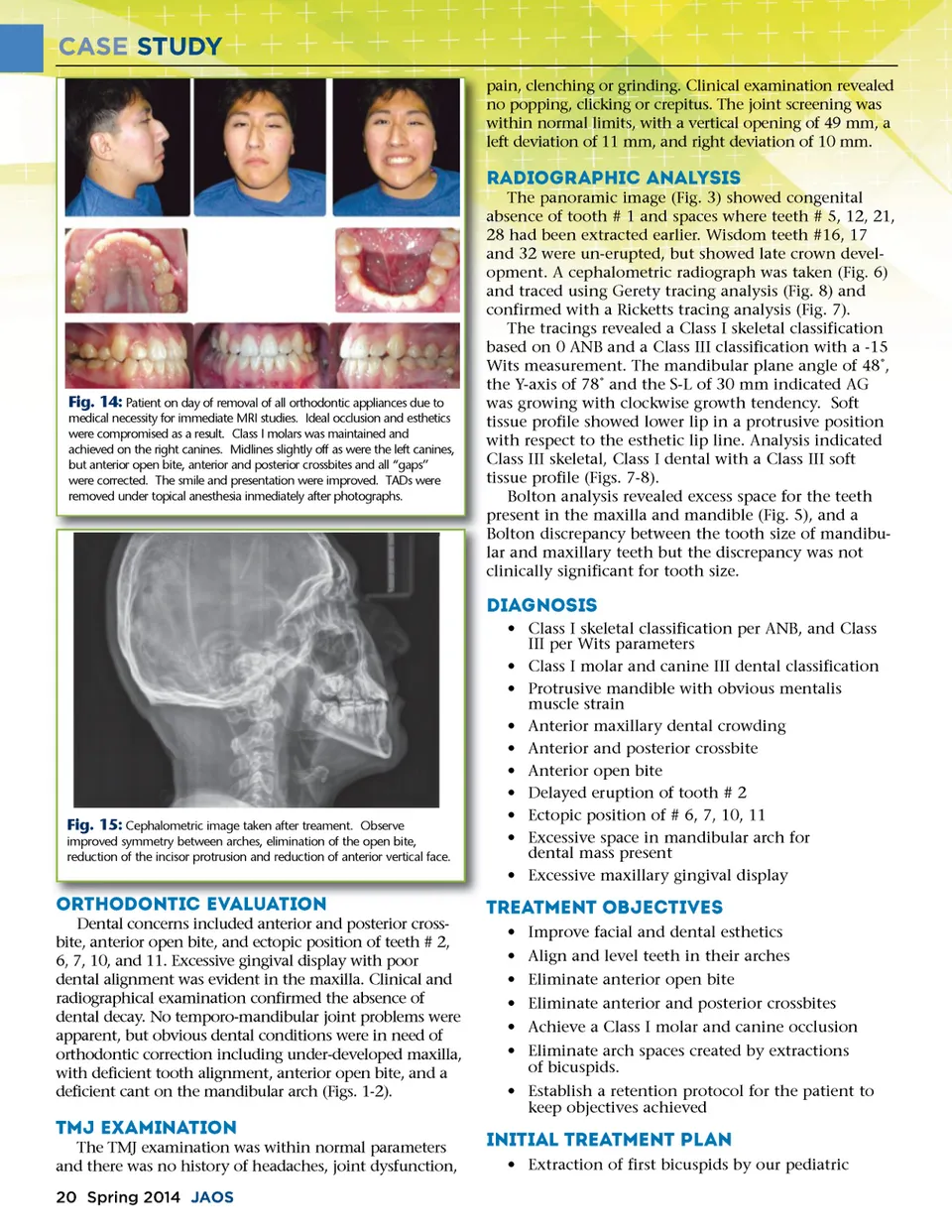
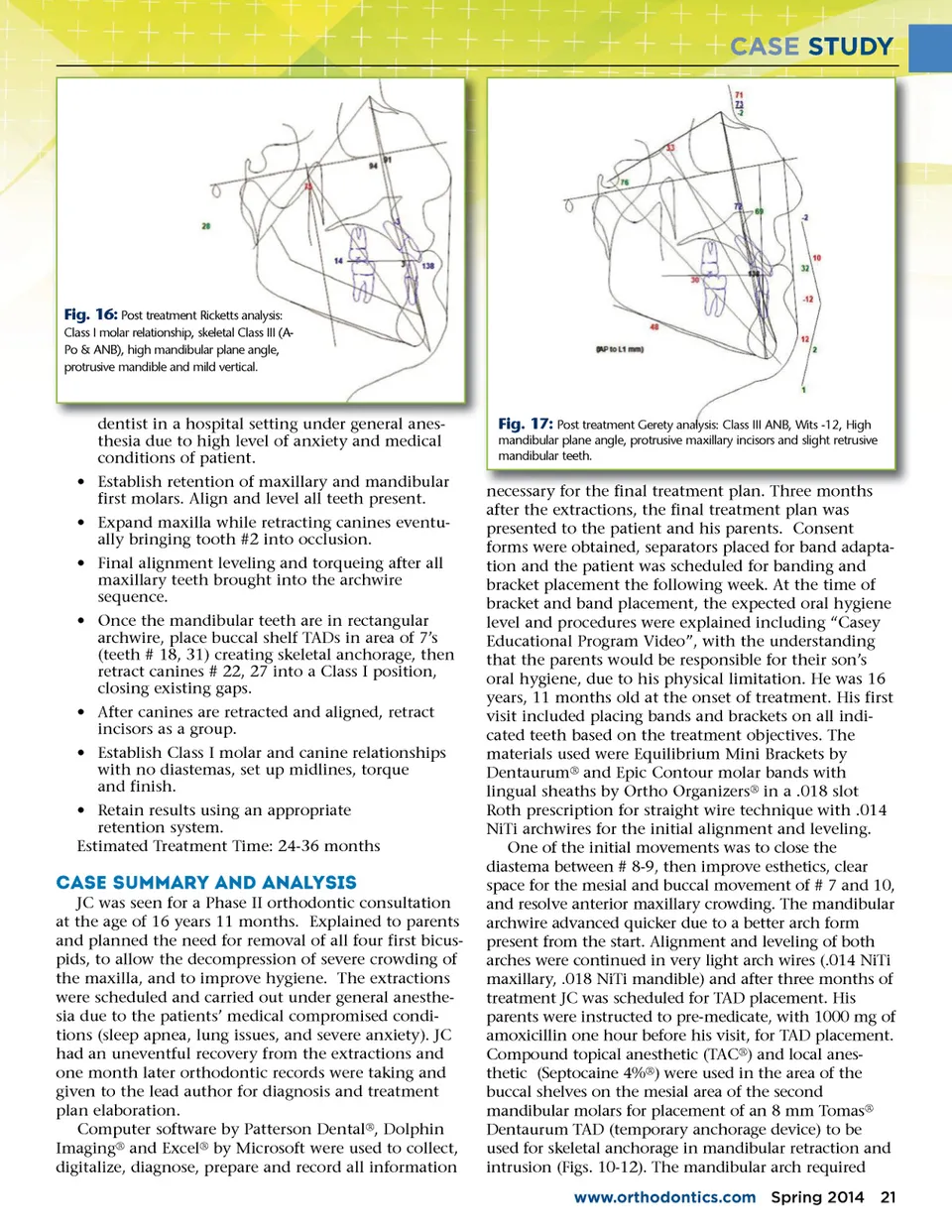
CASE STUDY pain, clenching or grinding. Clinical examination revealed no popping, clicking or crepitus. The joint screening was within normal limits, with a vertical opening of 49 mm, a left deviation of 11 mm, and right deviation of 10 mm. Radiographic Analysis The panoramic image (Fig. 3) showed congenital absence of tooth # 1 and spaces where teeth # 5, 12, 21, 28 had been extracted earlier. Wisdom teeth #16, 17 and 32 were un-erupted, but showed late crown devel-opment. A cephalometric radiograph was taken (Fig. 6) and traced using Gerety tracing analysis (Fig. 8) and confirmed with a Ricketts tracing analysis (Fig. 7). The tracings revealed a Class I skeletal classification based on 0 ANB and a Class III classification with a -15 Wits measurement. The mandibular plane angle of 48˚, the Y-axis of 78˚ and the S-L of 30 mm indicated AG was growing with clockwise growth tendency. Soft tissue profile showed lower lip in a protrusive position with respect to the esthetic lip line. Analysis indicated Class III skeletal, Class I dental with a Class III soft tissue profile (Figs. 7-8). Bolton analysis revealed excess space for the teeth present in the maxilla and mandible (Fig. 5), and a Bolton discrepancy between the tooth size of mandibu-lar and maxillary teeth but the discrepancy was not clinically significant for tooth size. Fig. 14: Patient on day of removal of all orthodontic appliances due to medical necessity for immediate MRI studies. Ideal occlusion and esthetics were compromised as a result. Class I molars was maintained and achieved on the right canines. Midlines slightly off as were the left canines, but anterior open bite, anterior and posterior crossbites and all “gaps” were corrected. The smile and presentation were improved. TADs were removed under topical anesthesia inmediately after photographs. Diagnosis • Class I skeletal classification per ANB, and Class III per Wits parameters • Class I molar and canine III dental classification • Protrusive mandible with obvious mentalis muscle strain • Anterior maxillary dental crowding • Anterior and posterior crossbite • Anterior open bite • Delayed eruption of tooth # 2 • Ectopic position of # 6, 7, 10, 11 • Excessive space in mandibular arch for dental mass present • Excessive maxillary gingival display Fig. 15: Cephalometric image taken after treament. Observe improved symmetry between arches, elimination of the open bite, reduction of the incisor protrusion and reduction of anterior vertical face. Orthodontic O r t h o d o n t i c evaluation e v a l u a t i o n Dental concerns included anterior and posterior cross-bite, anterior open bite, and ectopic position of teeth # 2, 6, 7, 10, and 11. Excessive gingival display with poor dental alignment was evident in the maxilla. Clinical and radiographical examination confirmed the absence of dental decay. No temporo-mandibular joint problems were apparent, but obvious dental conditions were in need of orthodontic correction including under-developed maxilla, with deficient tooth alignment, anterior open bite, and a deficient cant on the mandibular arch (Figs. 1-2). Treatment Objectives • Improve facial and dental esthetics • Align and level teeth in their arches • Eliminate anterior open bite • Eliminate anterior and posterior crossbites • Achieve a Class I molar and canine occlusion • Eliminate arch spaces created by extractions of bicuspids. • Establish a retention protocol for the patient to keep objectives achieved TMJ Examination The TMJ examination was within normal parameters and there was no history of headaches, joint dysfunction, 20 Spring 2014 JAOS Initial Treatment Plan • Extraction of first bicuspids by our pediatric
Journal of the American Orthodontic Society Spring 2014: Page 20