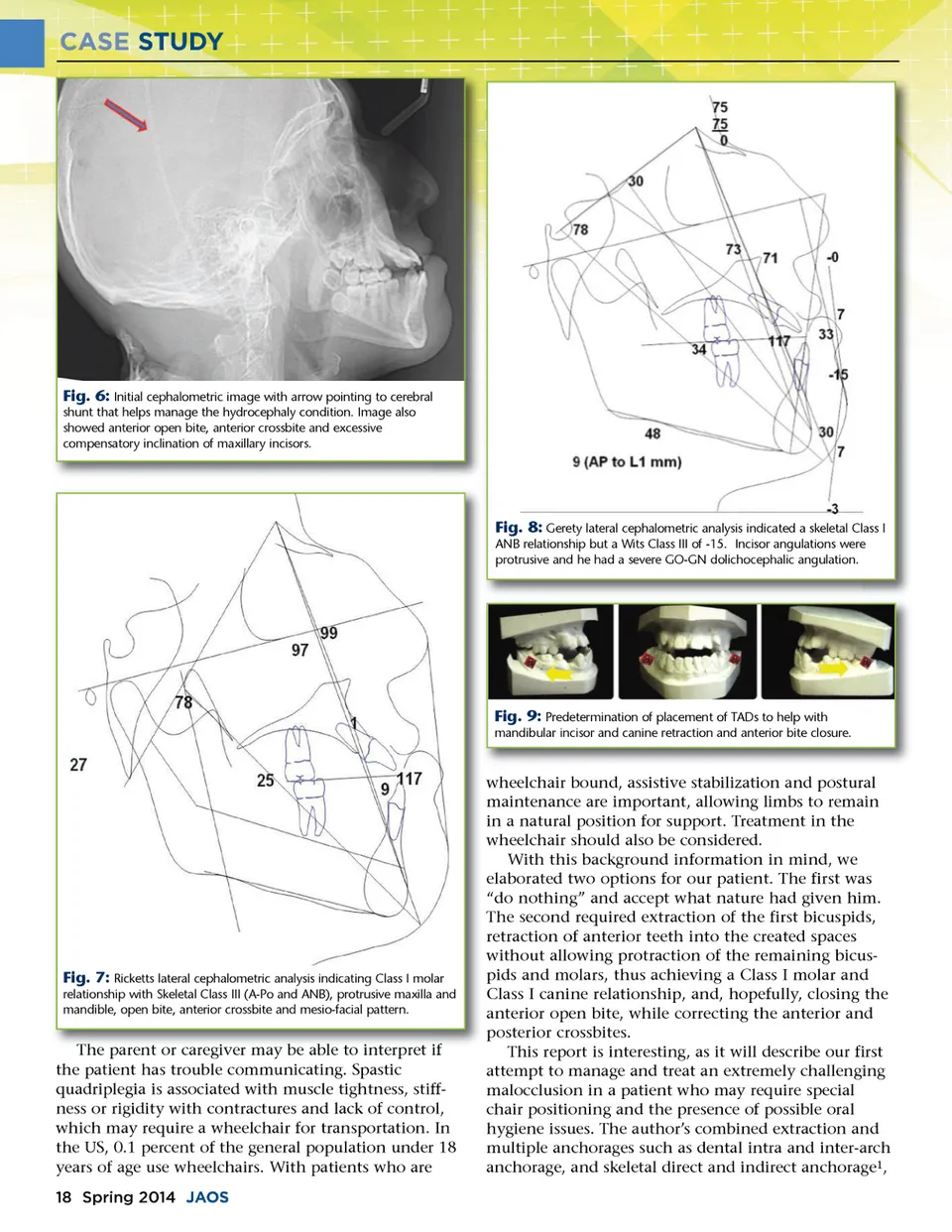
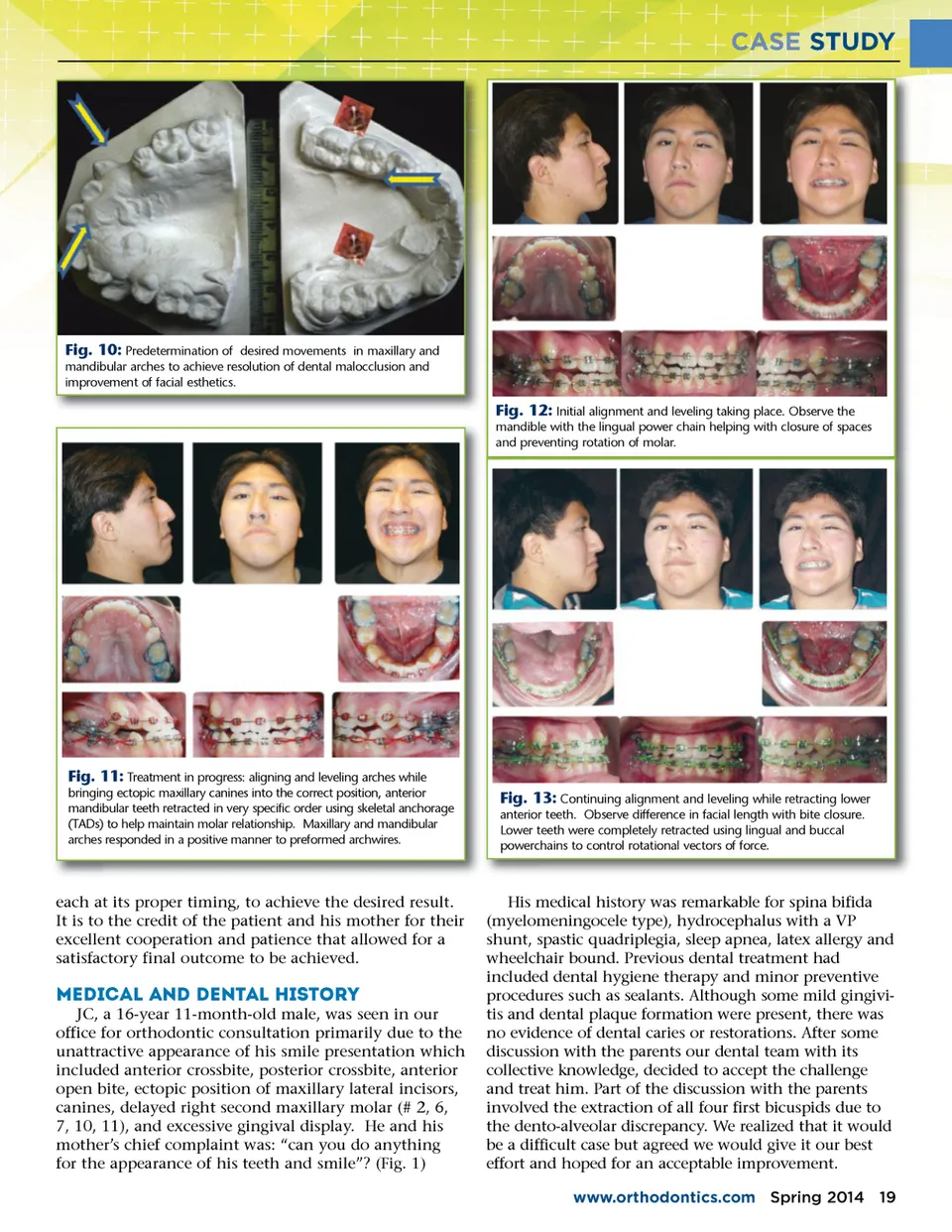
CASE STUDY Fig. 10: Predetermination of desired movements in maxillary and mandibular arches to achieve resolution of dental malocclusion and improvement of facial esthetics. Fig. 12: Initial alignment and leveling taking place. Observe the mandible with the lingual power chain helping with closure of spaces and preventing rotation of molar. Fig. 11: Treatment in progress: aligning and leveling arches while bringing ectopic maxillary canines into the correct position, anterior mandibular teeth retracted in very specific order using skeletal anchorage (TADs) to help maintain molar relationship. Maxillary and mandibular arches responded in a positive manner to preformed archwires. Fig. 13: Continuing alignment and leveling while retracting lower anterior teeth. Observe difference in facial length with bite closure. Lower teeth were completely retracted using lingual and buccal powerchains to control rotational vectors of force. each at its proper timing, to achieve the desired result. It is to the credit of the patient and his mother for their excellent cooperation and patience that allowed for a satisfactory final outcome to be achieved. Medical and Dental History JC, a 16-year 11-month-old male, was seen in our office for orthodontic consultation primarily due to the unattractive appearance of his smile presentation which included anterior crossbite, posterior crossbite, anterior open bite, ectopic position of maxillary lateral incisors, canines, delayed right second maxillary molar (# 2, 6, 7, 10, 11), and excessive gingival display. He and his mother’s chief complaint was: “can you do anything for the appearance of his teeth and smile”? (Fig. 1) His medical history was remarkable for spina bifida (myelomeningocele type), hydrocephalus with a VP shunt, spastic quadriplegia, sleep apnea, latex allergy and wheelchair bound. Previous dental treatment had included dental hygiene therapy and minor preventive procedures such as sealants. Although some mild gingivi-tis and dental plaque formation were present, there was no evidence of dental caries or restorations. After some discussion with the parents our dental team with its collective knowledge, decided to accept the challenge and treat him. Part of the discussion with the parents involved the extraction of all four first bicuspids due to the dento-alveolar discrepancy. We realized that it would be a difficult case but agreed we would give it our best effort and hoped for an acceptable improvement. www.orthodontics.com Spring 2014 19
Journal of the American Orthodontic Society Spring 2014: Page 19