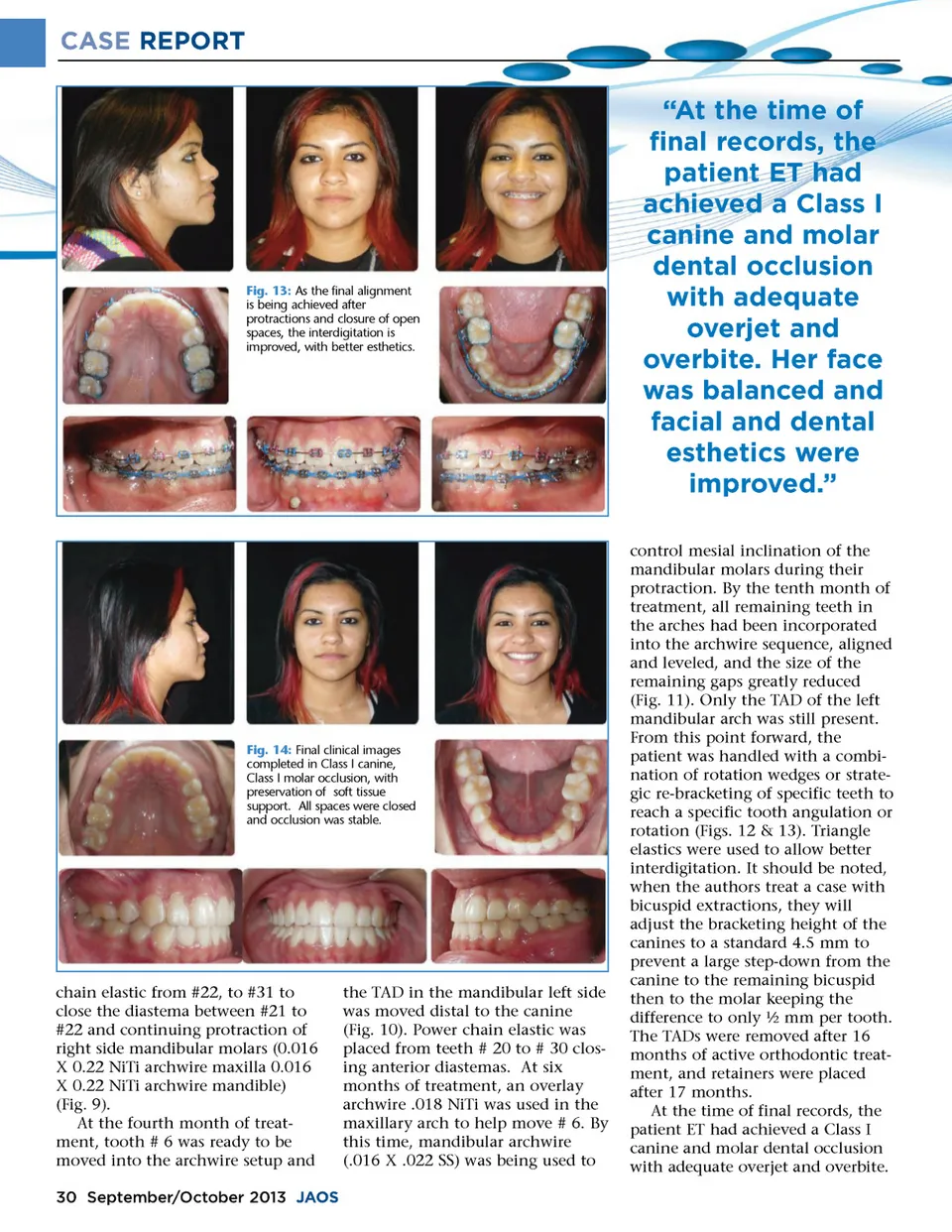
CASE REPORT Fig. 13: As the final alignment is being achieved after protractions and closure of open spaces, the interdigitation is improved, with better esthetics. “At the time of final records, the patient ET had achieved a Class I canine and molar dental occlusion with adequate overjet and overbite. Her face was balanced and facial and dental esthetics were improved.” control mesial inclination of the mandibular molars during their protraction. By the tenth month of treatment, all remaining teeth in the arches had been incorporated into the archwire sequence, aligned and leveled, and the size of the remaining gaps greatly reduced (Fig. 11). Only the TAD of the left mandibular arch was still present. From this point forward, the patient was handled with a combi-nation of rotation wedges or strate-gic re-bracketing of specific teeth to reach a specific tooth angulation or rotation (Figs. 12 & 13). Triangle elastics were used to allow better interdigitation. It should be noted, when the authors treat a case with bicuspid extractions, they will adjust the bracketing height of the canines to a standard 4.5 mm to prevent a large step-down from the canine to the remaining bicuspid then to the molar keeping the difference to only ½ mm per tooth. The TADs were removed after 16 months of active orthodontic treat-ment, and retainers were placed after 17 months. At the time of final records, the patient ET had achieved a Class I canine and molar dental occlusion with adequate overjet and overbite. Fig. 14: Final clinical images completed in Class I canine, Class I molar occlusion, with preservation of soft tissue support. All spaces were closed and occlusion was stable. chain elastic from #22, to #31 to close the diastema between #21 to #22 and continuing protraction of right side mandibular molars (0.016 X 0.22 NiTi archwire maxilla 0.016 X 0.22 NiTi archwire mandible) (Fig. 9). At the fourth month of treat-ment, tooth # 6 was ready to be moved into the archwire setup and 30 September/October 2013 JAOS the TAD in the mandibular left side was moved distal to the canine (Fig. 10). Power chain elastic was placed from teeth # 20 to # 30 clos-ing anterior diastemas. At six months of treatment, an overlay archwire .018 NiTi was used in the maxillary arch to help move # 6. By this time, mandibular archwire (.016 X .022 SS) was being used to
Journal of the American Orthodontic Society September-October 2013: Page 30