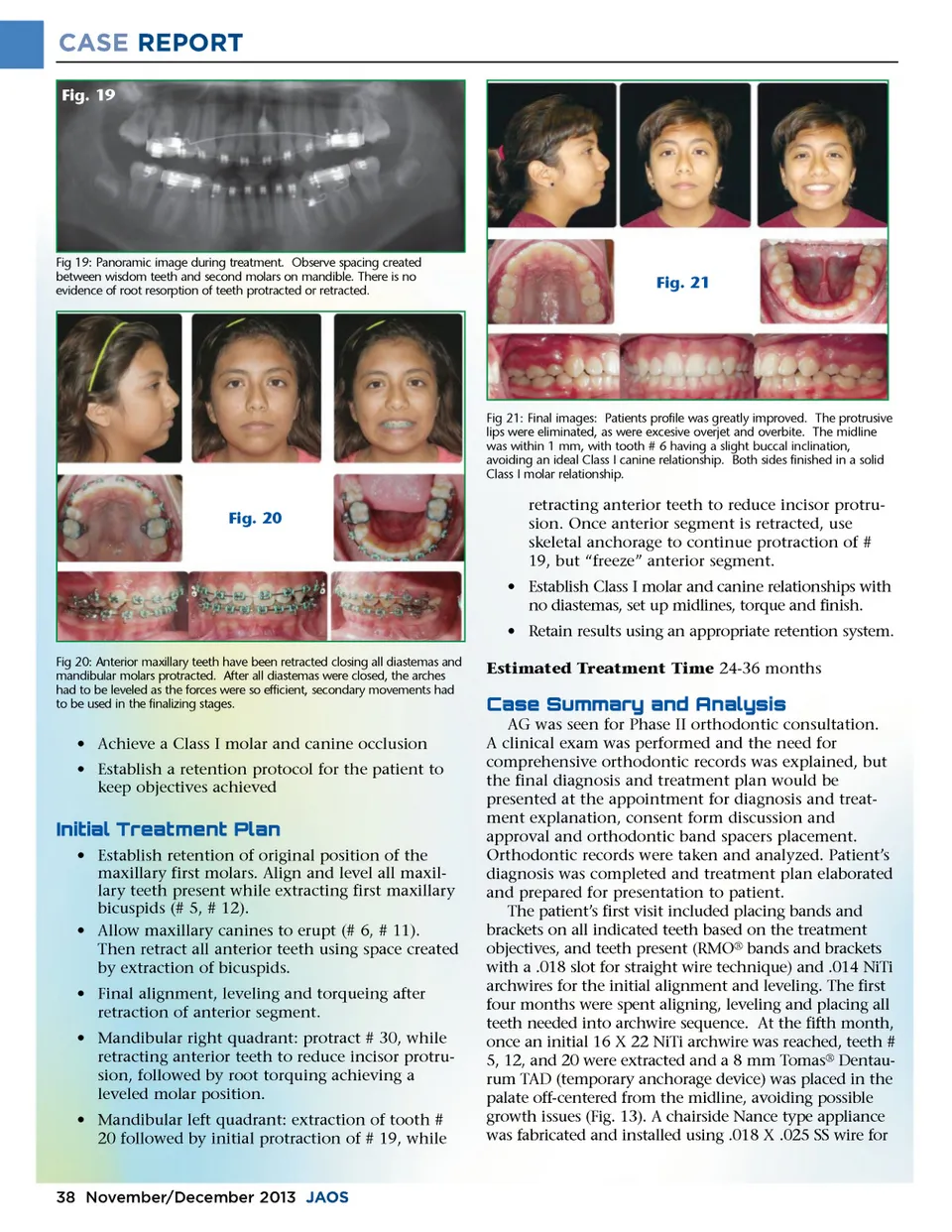
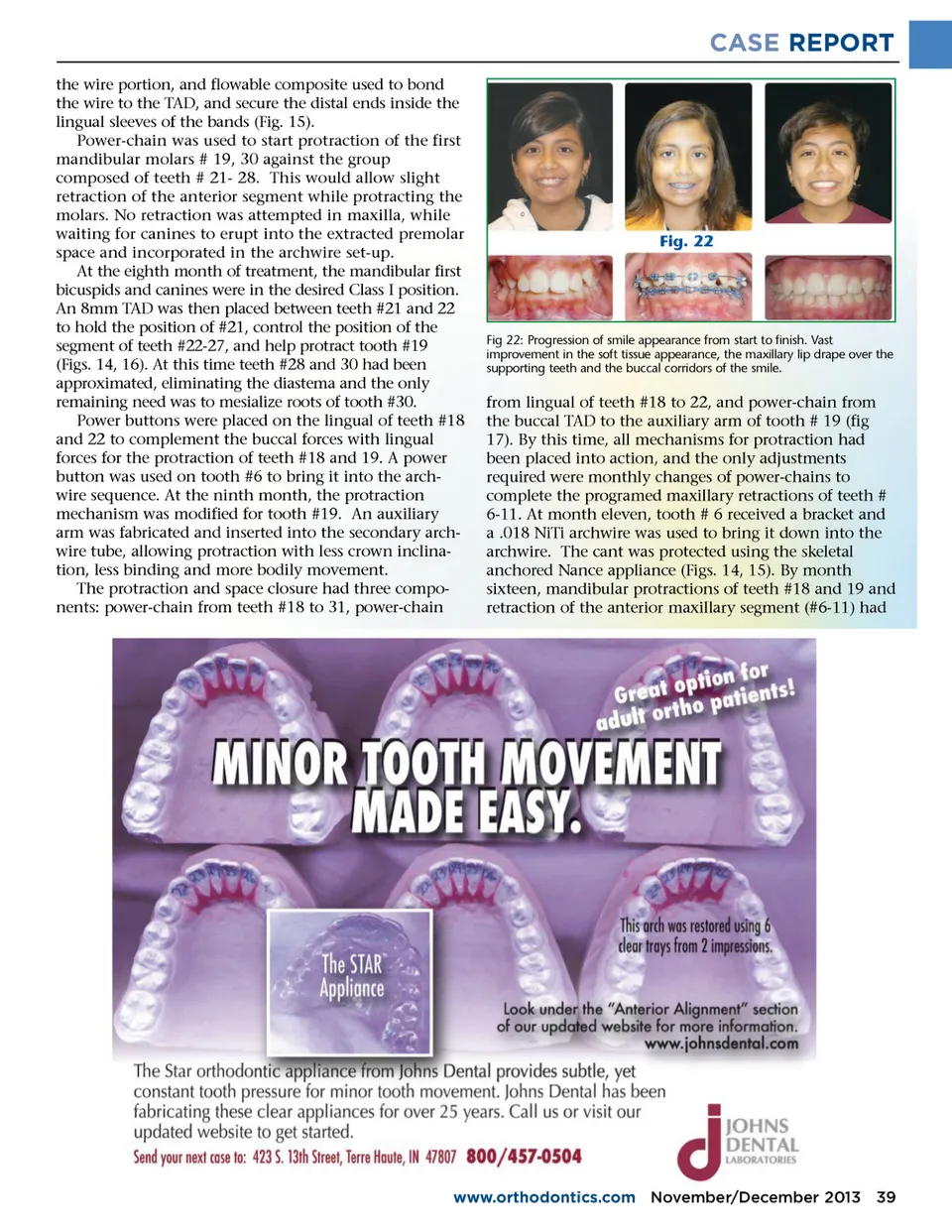
CASE REPORT Fig. 19 Fig 19: Panoramic image during treatment. Observe spacing created between wisdom teeth and second molars on mandible. There is no evidence of root resorption of teeth protracted or retracted. Fig. 21 Fig 21: Final images: Patients profile was greatly improved. The protrusive lips were eliminated, as were excesive overjet and overbite. The midline was within 1 mm, with tooth # 6 having a slight buccal inclination, avoiding an ideal Class I canine relationship. Both sides finished in a solid Class I molar relationship. Fig. 20 retracting anterior teeth to reduce incisor protru-sion. Once anterior segment is retracted, use skeletal anchorage to continue protraction of # 19, but “freeze” anterior segment. • Establish Class I molar and canine relationships with no diastemas, set up midlines, torque and finish. • Retain results using an appropriate retention system. Fig 20: Anterior maxillary teeth have been retracted closing all diastemas and mandibular molars protracted. After all diastemas were closed, the arches had to be leveled as the forces were so efficient, secondary movements had to be used in the finalizing stages. Estimated Treatment Time 24-36 months $e;!f;�d;a;a;$d;f;$"f;�b;"$b;e;#e; AG was seen for Phase II orthodontic consultation. A clinical exam was performed and the need for comprehensive orthodontic records was explained, but the final diagnosis and treatment plan would be presented at the appointment for diagnosis and treat-ment explanation, consent form discussion and approval and orthodontic band spacers placement. Orthodontic records were taken and analyzed. Patient’s diagnosis was completed and treatment plan elaborated and prepared for presentation to patient. The patient’s first visit included placing bands and brackets on all indicated teeth based on the treatment objectives, and teeth present (RMO ® bands and brackets with a .018 slot for straight wire technique) and .014 NiTi archwires for the initial alignment and leveling. The first four months were spent aligning, leveling and placing all teeth needed into archwire sequence. At the fifth month, once an initial 16 X 22 NiTi archwire was reached, teeth # 5, 12, and 20 were extracted and a 8 mm Tomas ® Dentau-rum TAD (temporary anchorage device) was placed in the palate off-centered from the midline, avoiding possible growth issues (Fig. 13). A chairside Nance type appliance was fabricated and installed using .018 X .025 SS wire for • Achieve a Class I molar and canine occlusion • Establish a retention protocol for the patient to keep objectives achieved "# #$b;f;d;!$ a;!" f;b;$" • Establish retention of original position of the maxillary first molars. Align and level all maxil-lary teeth present while extracting first maxillary bicuspids (# 5, # 12). • Allow maxillary canines to erupt (# 6, # 11). Then retract all anterior teeth using space created by extraction of bicuspids. • Final alignment, leveling and torqueing after retraction of anterior segment. • Mandibular right quadrant: protract # 30, while retracting anterior teeth to reduce incisor protru-sion, followed by root torquing achieving a leveled molar position. • Mandibular left quadrant: extraction of tooth # 20 followed by initial protraction of # 19, while 38 November/December 2013 JAOS
Journal of the American Orthodontic Society November-December 2013: Page 38