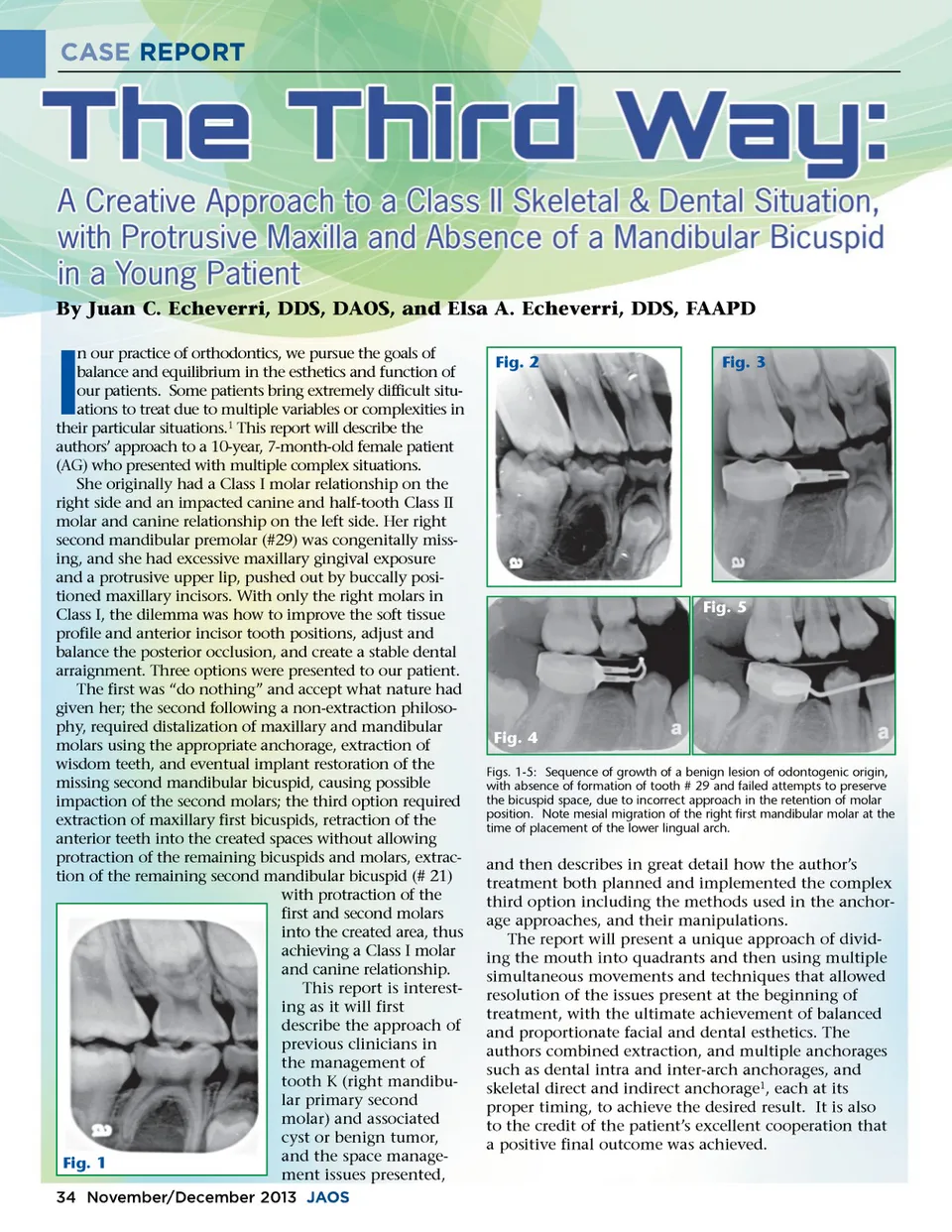
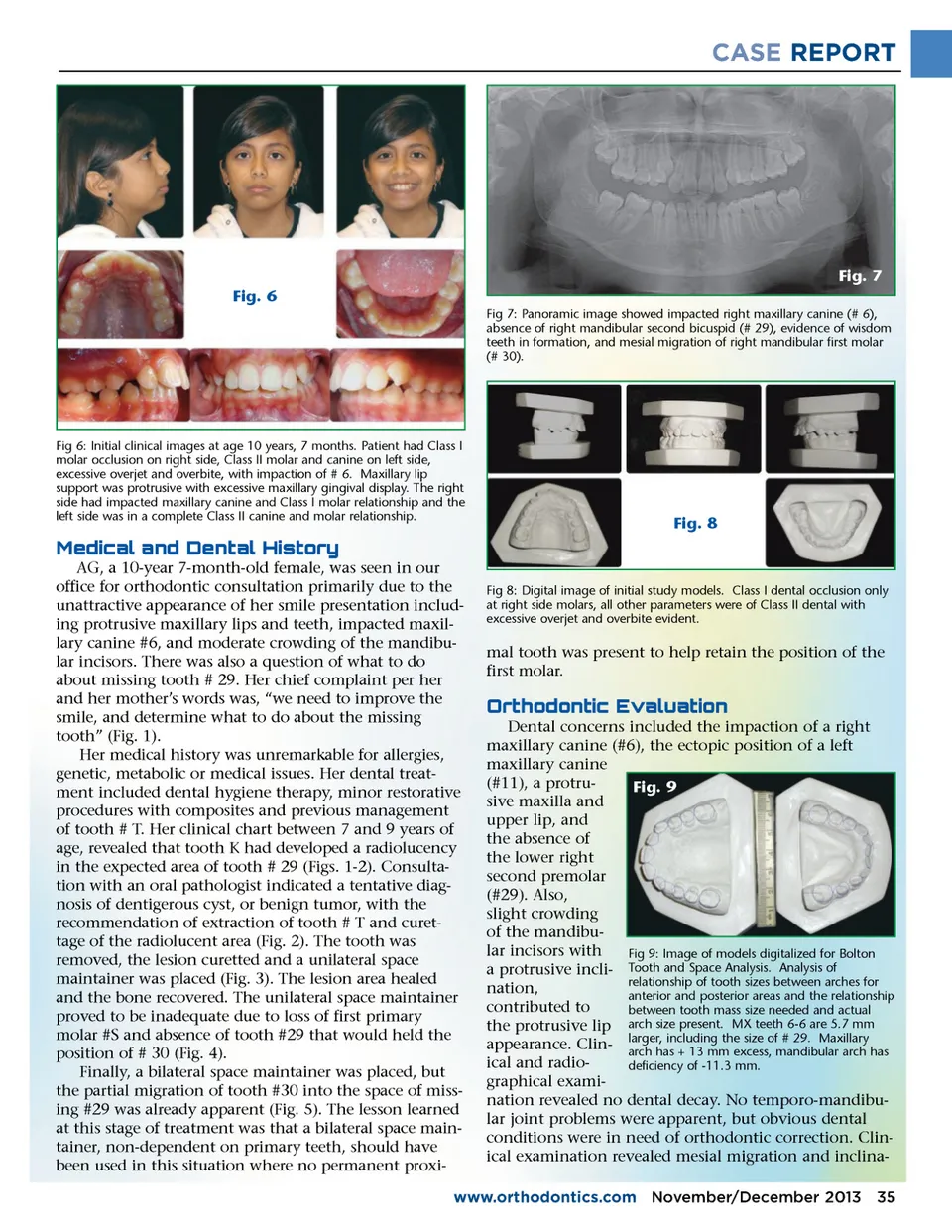
CASE REPORT Fig. 7 Fig. 6 Fig 7: Panoramic image showed impacted right maxillary canine (# 6), absence of right mandibular second bicuspid (# 29), evidence of wisdom teeth in formation, and mesial migration of right mandibular first molar (# 30). Fig 6: Initial clinical images at age 10 years, 7 months. Patient had Class I molar occlusion on right side, Class II molar and canine on left side, excessive overjet and overbite, with impaction of # 6. Maxillary lip support was protrusive with excessive maxillary gingival display. The right side had impacted maxillary canine and Class I molar relationship and the left side was in a complete Class II canine and molar relationship. Fig. 8 !#$b;f;$"f;!" $b;f;#e; c;d; AG, a 10-year 7-month-old female, was seen in our office for orthodontic consultation primarily due to the unattractive appearance of her smile presentation includ-ing protrusive maxillary lips and teeth, impacted maxil-lary canine #6, and moderate crowding of the mandibu-lar incisors. There was also a question of what to do about missing tooth # 29. Her chief complaint per her and her mother’s words was, “we need to improve the smile, and determine what to do about the missing tooth” (Fig. 1). Her medical history was unremarkable for allergies, genetic, metabolic or medical issues. Her dental treat-ment included dental hygiene therapy, minor restorative procedures with composites and previous management of tooth # T. Her clinical chart between 7 and 9 years of age, revealed that tooth K had developed a radiolucency in the expected area of tooth # 29 (Figs. 1-2). Consulta-tion with an oral pathologist indicated a tentative diag-nosis of dentigerous cyst, or benign tumor, with the recommendation of extraction of tooth # T and curet-tage of the radiolucent area (Fig. 2). The tooth was removed, the lesion curetted and a unilateral space maintainer was placed (Fig. 3). The lesion area healed and the bone recovered. The unilateral space maintainer proved to be inadequate due to loss of first primary molar #S and absence of tooth #29 that would held the position of # 30 (Fig. 4). Finally, a bilateral space maintainer was placed, but the partial migration of tooth #30 into the space of miss-ing #29 was already apparent (Fig. 5). The lesson learned at this stage of treatment was that a bilateral space main-tainer, non-dependent on primary teeth, should have been used in this situation where no permanent proxi-Fig 8: Digital image of initial study models. Class I dental occlusion only at right side molars, all other parameters were of Class II dental with excessive overjet and overbite evident. mal tooth was present to help retain the position of the first molar. d; �e;c;c;" #f; �c;$b;�d;$ #c;" Dental concerns included the impaction of a right maxillary canine (#6), the ectopic position of a left maxillary canine (#11), a protru-Fig. 9 sive maxilla and upper lip, and the absence of the lower right second premolar (#29). Also, slight crowding of the mandibu-lar incisors with Fig 9: Image of models digitalized for Bolton a protrusive incli-Tooth and Space Analysis. Analysis of relationship of tooth sizes between arches for nation, anterior and posterior areas and the relationship contributed to between tooth mass size needed and actual the protrusive lip arch size present. MX teeth 6-6 are 5.7 mm including the size of # 29. Maxillary appearance. Clin-larger, arch has + 13 mm excess, mandibular arch has ical and radio-deficiency of -11.3 mm. graphical exami-nation revealed no dental decay. No temporo-mandibu-lar joint problems were apparent, but obvious dental conditions were in need of orthodontic correction. Clin-ical examination revealed mesial migration and inclina-www.orthodontics.com November/December 2013 35
Journal of the American Orthodontic Society November-December 2013: Page 35