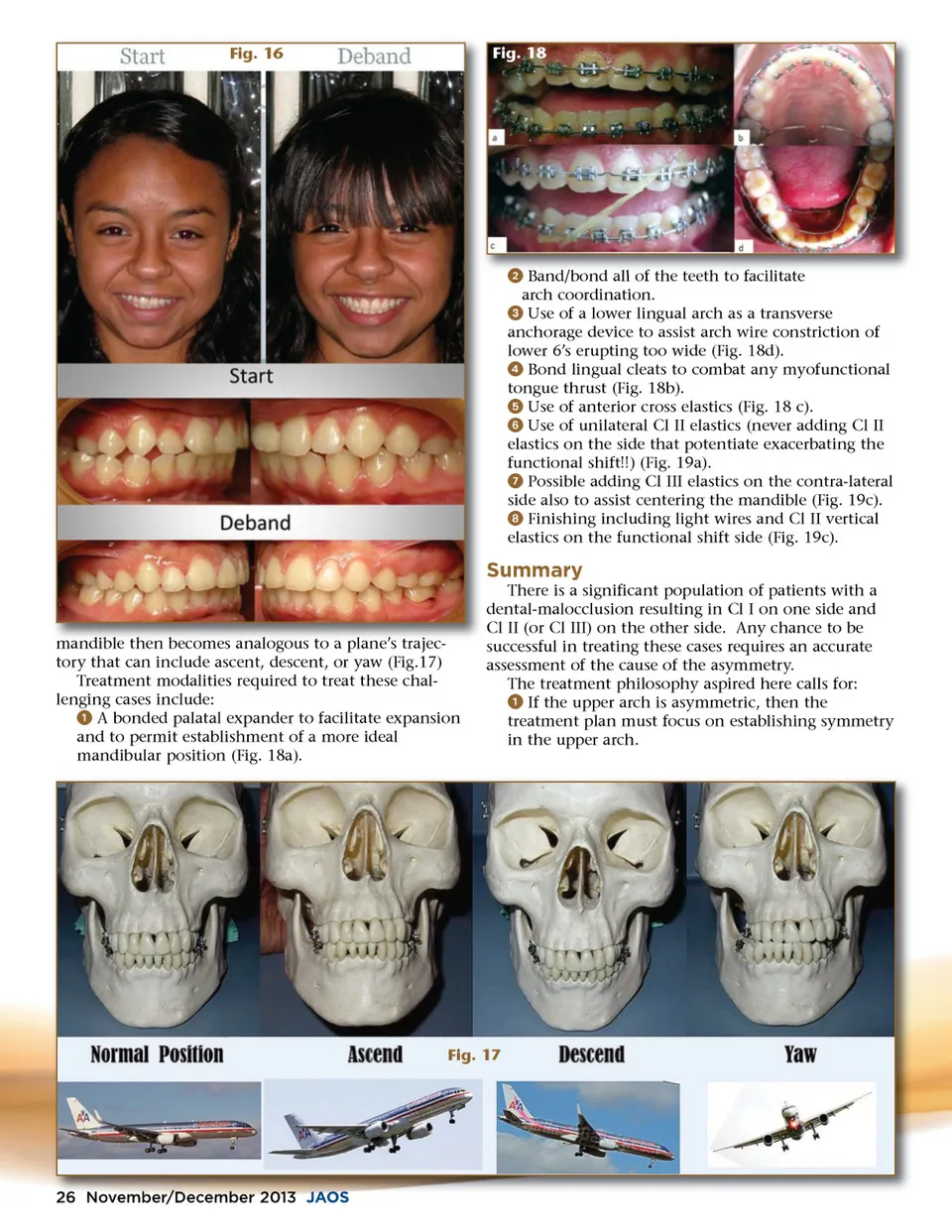
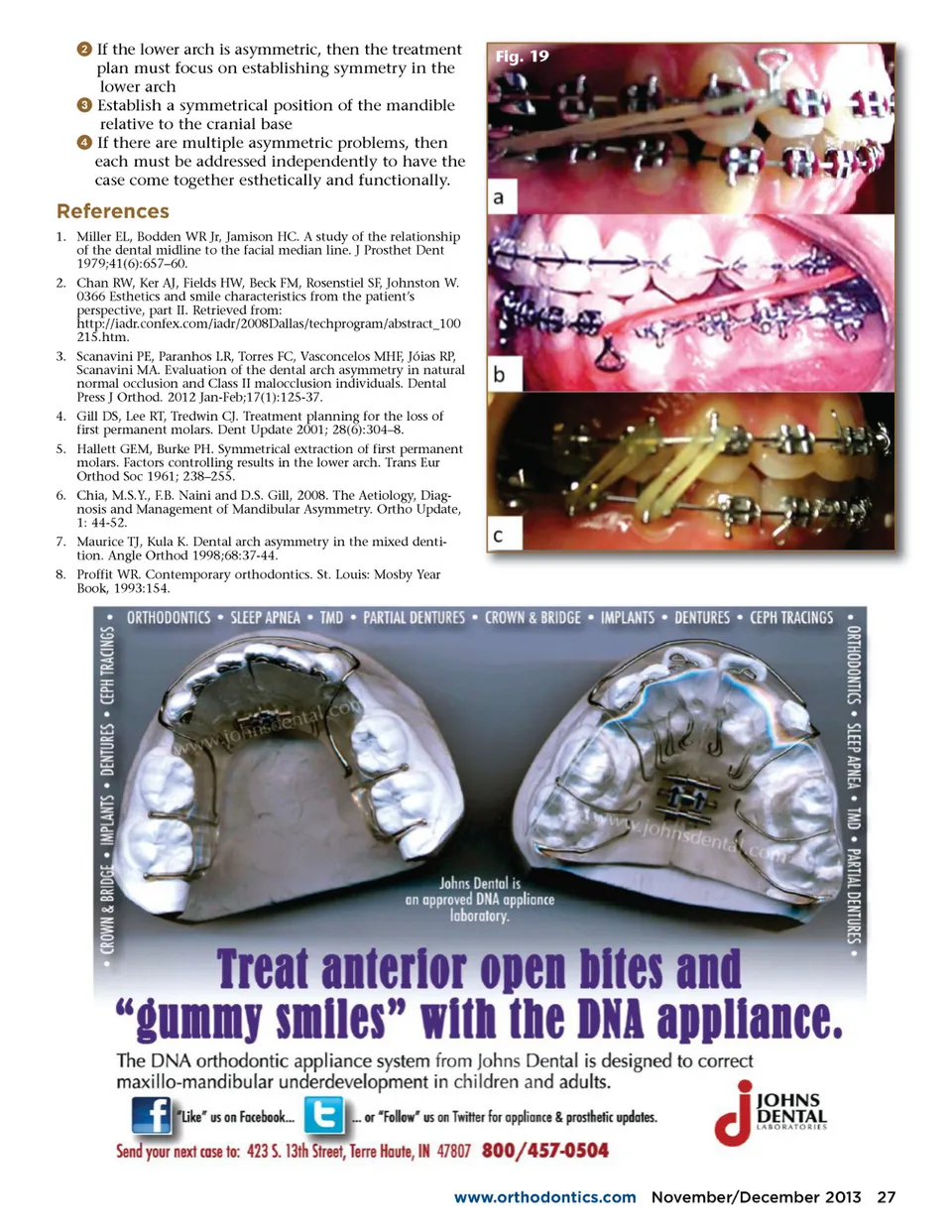
Fig. 16 Fig. 18 ᕢ Band/bond all of the teeth to facilitate arch coordination. ᕣ Use of a lower lingual arch as a transverse anchorage device to assist arch wire constriction of lower 6’s erupting too wide (Fig. 18d). ᕤ Bond lingual cleats to combat any myofunctional tongue thrust (Fig. 18b). ᕥ Use of anterior cross elastics (Fig. 18 c). ᕦ Use of unilateral Cl II elastics (never adding Cl II elastics on the side that potentiate exacerbating the functional shift!!) (Fig. 19a). ᕧ Possible adding Cl III elastics on the contra-lateral side also to assist centering the mandible (Fig. 19c). ᕨ Finishing including light wires and Cl II vertical elastics on the functional shift side (Fig. 19c). Summary There is a significant population of patients with a dental-malocclusion resulting in Cl I on one side and Cl II (or Cl III) on the other side. Any chance to be successful in treating these cases requires an accurate assessment of the cause of the asymmetry. The treatment philosophy aspired here calls for: ᕡ If the upper arch is asymmetric, then the treatment plan must focus on establishing symmetry in the upper arch. mandible then becomes analogous to a plane’s trajec trajec-tory that can include ascent, descent, or yaw (Fig.17) Treatment modalities required to treat these chal-lenging cases include: ᕡ A bonded palatal expander to facilitate expansion and to permit establishment of a more ideal mandibular position (Fig. 18a). Fig. 17 26 November/December November/ r December 2013 JAOS
Journal of the American Orthodontic Society November-December 2013: Page 26