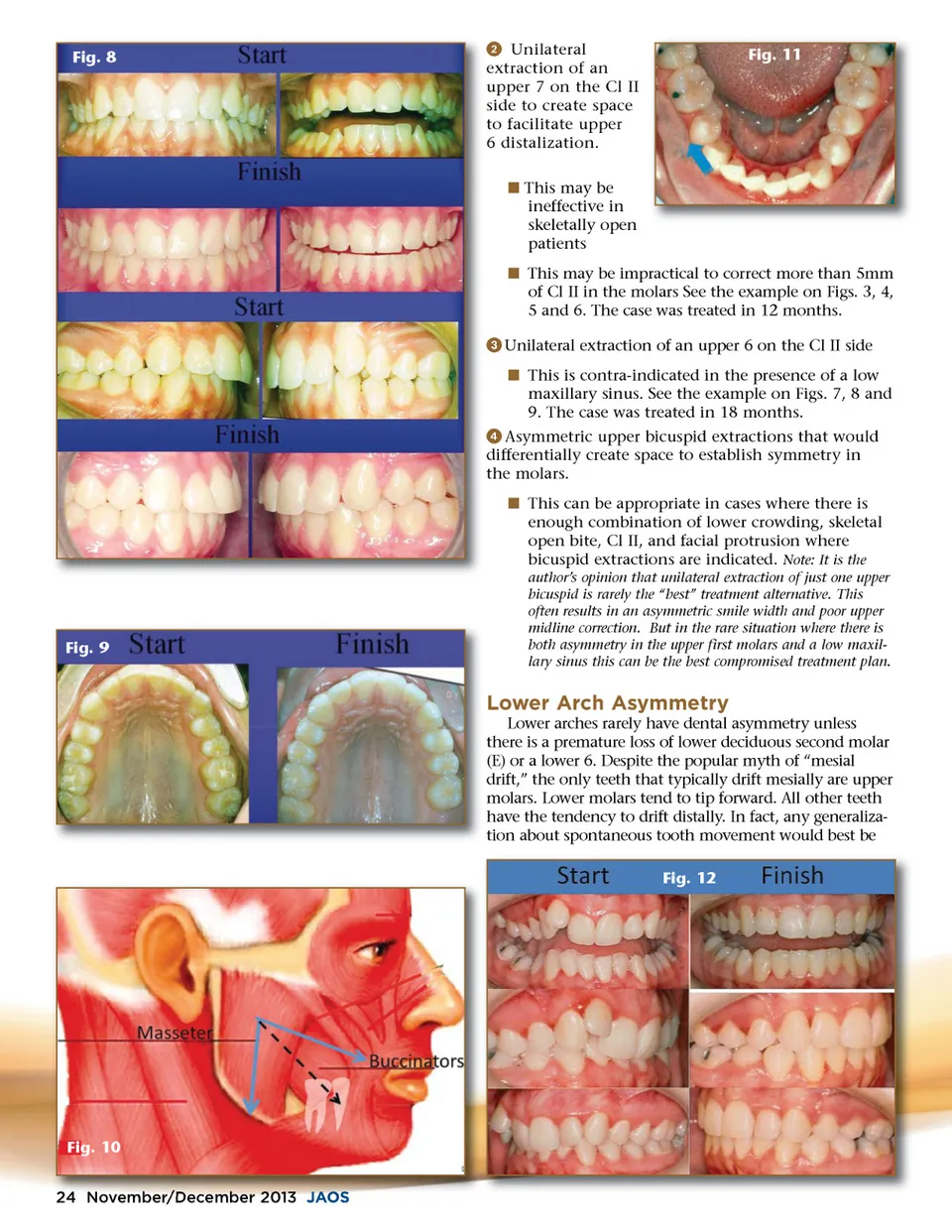
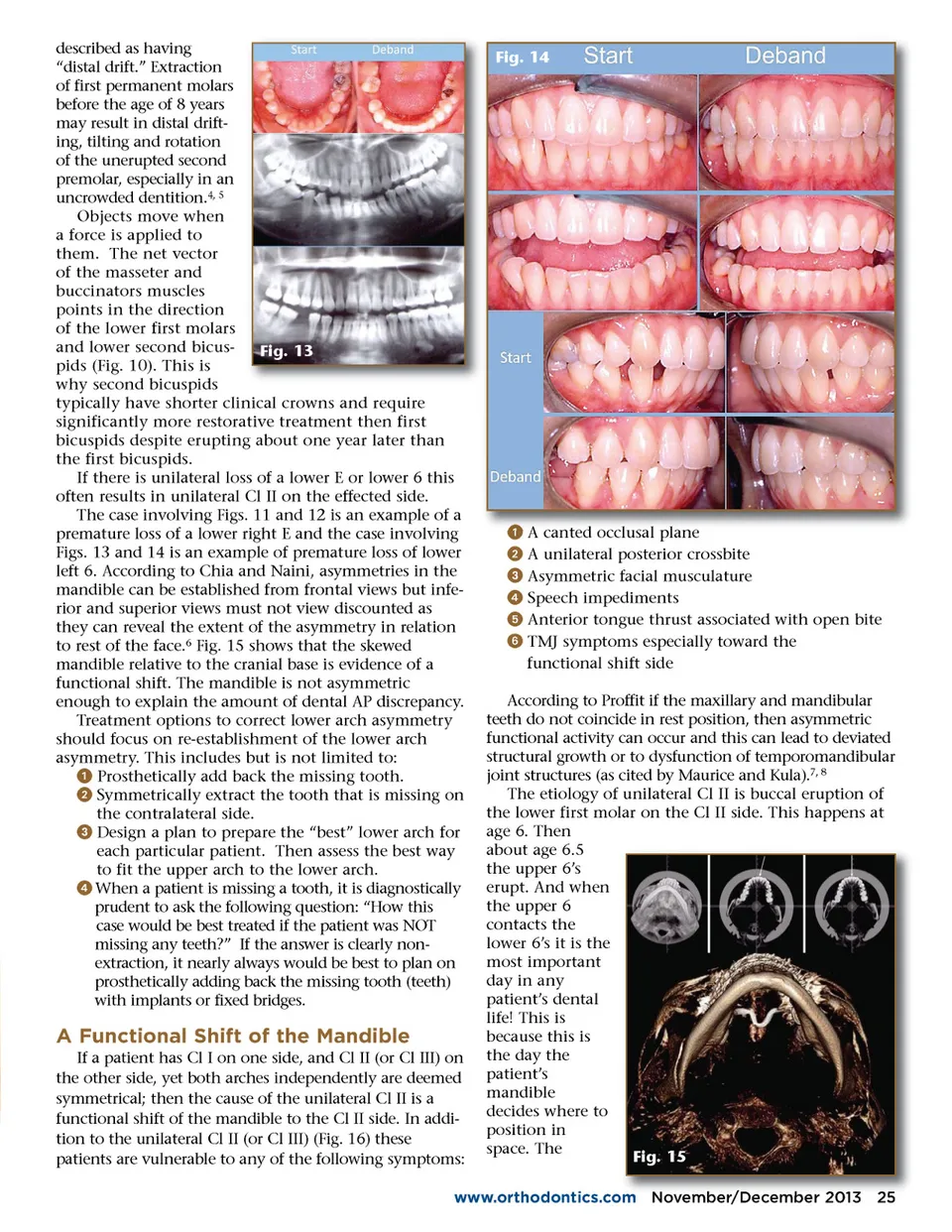
described as having “distal drift.” Extraction of first permanent molars before the age of 8 years may result in distal drift-ing, tilting and rotation of the unerupted second premolar, especially in an uncrowded dentition. 4, 5 Objects move when a force is applied to them. The net vector of the masseter and buccinators muscles points in the direction of the lower first molars and lower second bicus-Fig. 13 pids (Fig. 10). This is why second bicuspids typically have shorter clinical crowns and require significantly more restorative treatment then first bicuspids despite erupting about one year later than the first bicuspids. If there is unilateral loss of a lower E or lower 6 this often results in unilateral Cl II on the effected side. The case involving Figs. 11 and 12 is an example of a premature loss of a lower right E and the case involving Figs. 13 and 14 is an example of premature loss of lower left 6. According to Chia and Naini, asymmetries in the mandible can be established from frontal views but infe-rior and superior views must not view discounted as they can reveal the extent of the asymmetry in relation to rest of the face. 6 Fig. 15 shows that the skewed mandible relative to the cranial base is evidence of a functional shift. The mandible is not asymmetric enough to explain the amount of dental AP discrepancy. Treatment options to correct lower arch asymmetry should focus on re-establishment of the lower arch asymmetry. This includes but is not limited to: ᕡ Prosthetically add back the missing tooth. ᕢ Symmetrically extract the tooth that is missing on the contralateral side. ᕣ Design a plan to prepare the “best” lower arch for each particular patient. Then assess the best way to fit the upper arch to the lower arch. ᕤ When a patient is missing a tooth, it is diagnostically prudent to ask the following question: “How this case would be best treated if the patient was NOT missing any teeth?” If the answer is clearly non-extraction, it nearly always would be best to plan on prosthetically adding back the missing tooth (teeth) with implants or fixed bridges. Fig. 14 ᕡ ᕢ ᕣ ᕤ ᕥ ᕦ A canted occlusal plane A unilateral posterior crossbite Asymmetric facial musculature Speech impediments Anterior tongue thrust associated with open bite TMJ symptoms especially toward the functional shift side A Functional Shift of the Mandible If a patient has Cl I on one side, and Cl II (or Cl III) on the other side, yet both arches independently are deemed symmetrical; then the cause of the unilateral Cl II is a functional shift of the mandible to the Cl II side. In addi-tion to the unilateral Cl II (or Cl III) (Fig. 16) these patients are vulnerable to any of the following symptoms: According to Proffit if the maxillary and mandibular teeth do not coincide in rest position, then asymmetric functional activity can occur and this can lead to deviated structural growth or to dysfunction of temporomandibular joint structures (as cited by Maurice and Kula). 7, 8 The etiology of unilateral Cl II is buccal eruption of the lower first molar on the Cl II side. This happens at age 6. Then about age 6.5 the upper 6’s erupt. And when the upper 6 contacts the lower 6’s it is the most important day in any patient’s dental life! This is because this is the day the patient’s mandible decides where to position in space. The Fig. 15 www.orthodontics.com om November/ November/December r December 2013 25
Journal of the American Orthodontic Society November-December 2013: Page 25