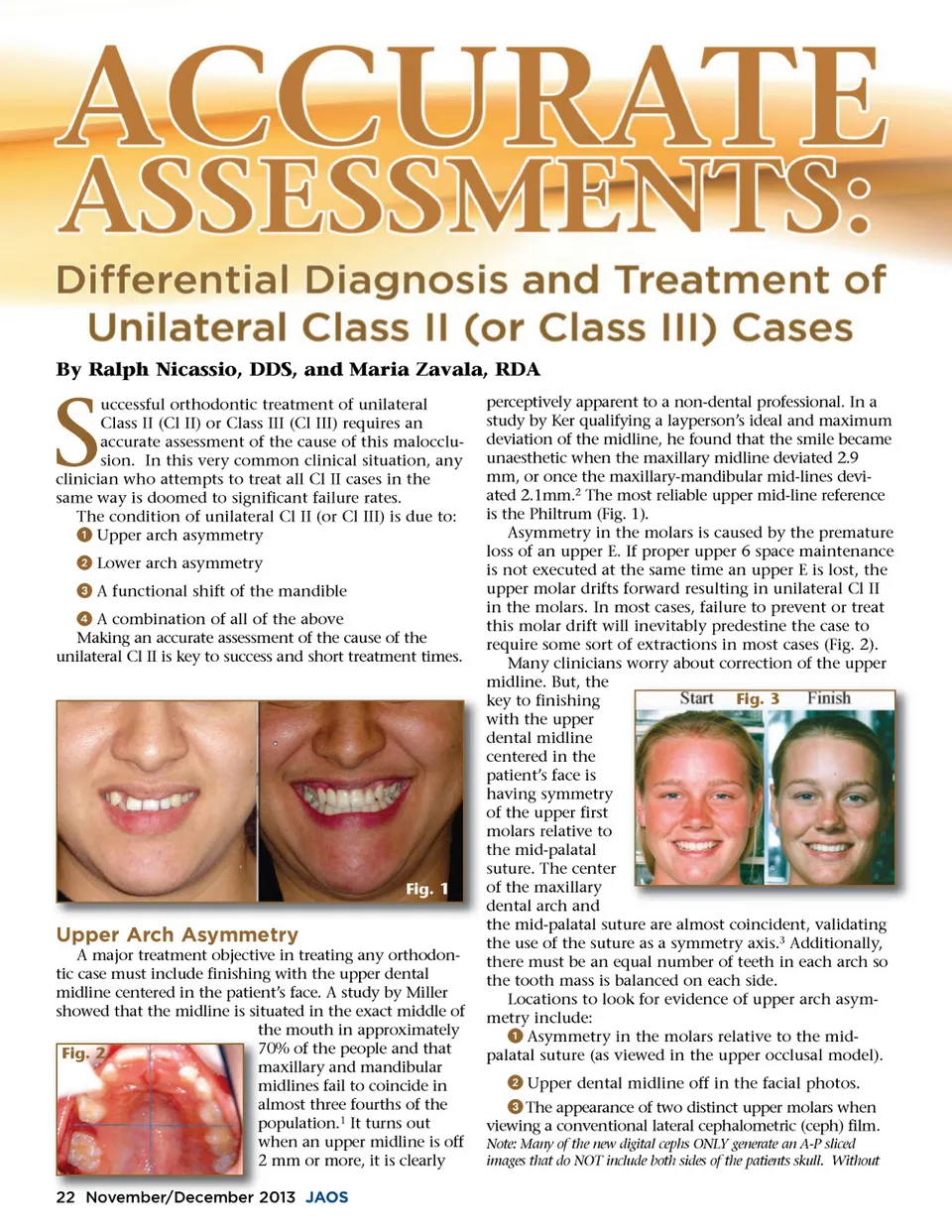
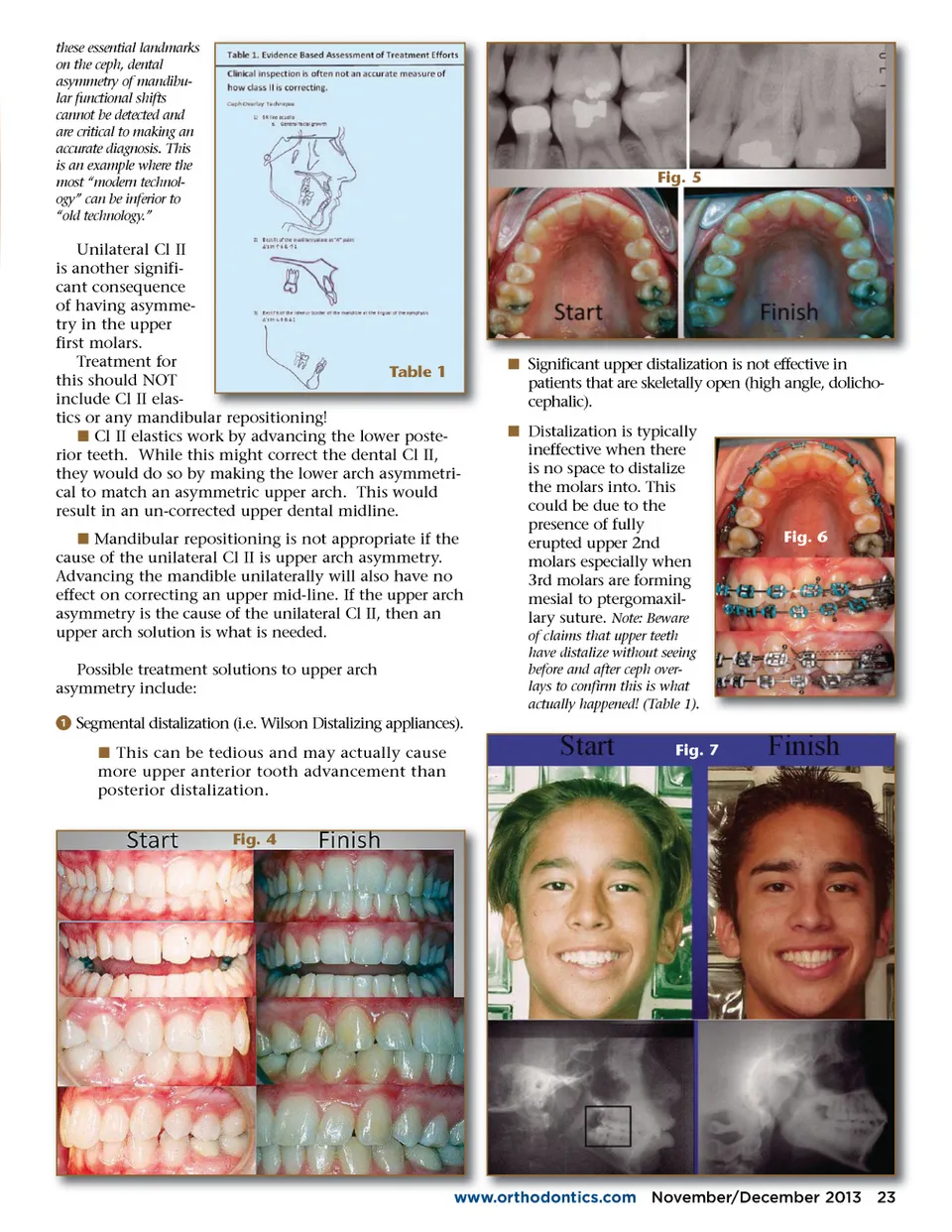
these essential landmarks on the ceph, dental asymmetry of mandibu-lar functional shifts cannot be detected and are critical to making an accurate diagnosis. This is an example where the most “modern technol-ogy” can be inferior to “old technology.” Fig. 5 Unilateral Cl II is another signifi-cant consequence of having asymme-try in the upper first molars. Treatment for Table 1 this should NOT include Cl II elas-tics or any mandibular repositioning! iti i ! í Cl II elastics work by advancing the lower poste-rior teeth. While this might correct the dental Cl II, they would do so by making the lower arch asymmetri-cal to match an asymmetric upper arch. This would result in an un-corrected upper dental midline. í Mandibular repositioning is not appropriate if the cause of the unilateral Cl II is upper arch asymmetry. Advancing the mandible unilaterally will also have no effect on correcting an upper mid-line. If the upper arch asymmetry is the cause of the unilateral Cl II, then an upper arch solution is what is needed. Possible treatment solutions to upper arch asymmetry include: ᕡ Segmental distalization (i.e. Wilson Distalizing appliances). í This can be tedious and may actually cause more upper anterior tooth advancement than posterior distalization. Fig. 4 í Significant Si ifi f t upper distalization di t li ti is i not t effective f ti in ff i patients that are skeletally open (high angle, dolicho-cephalic). í Distalization is typically ineffective when there is no space to distalize the molars into. This could be due to the presence of fully erupted upper 2nd molars especially when 3rd molars are forming mesial to ptergomaxil-lary suture. Note: Beware of claims that upper teeth have distalize without seeing before and after ceph over-lays to confirm this is what actually happened! (Table 1). Fig. 6 Fig. 7 www.orthodontics.com ww ww orthodontics com November/ November/December r December 2013 23
Journal of the American Orthodontic Society November-December 2013: Page 23