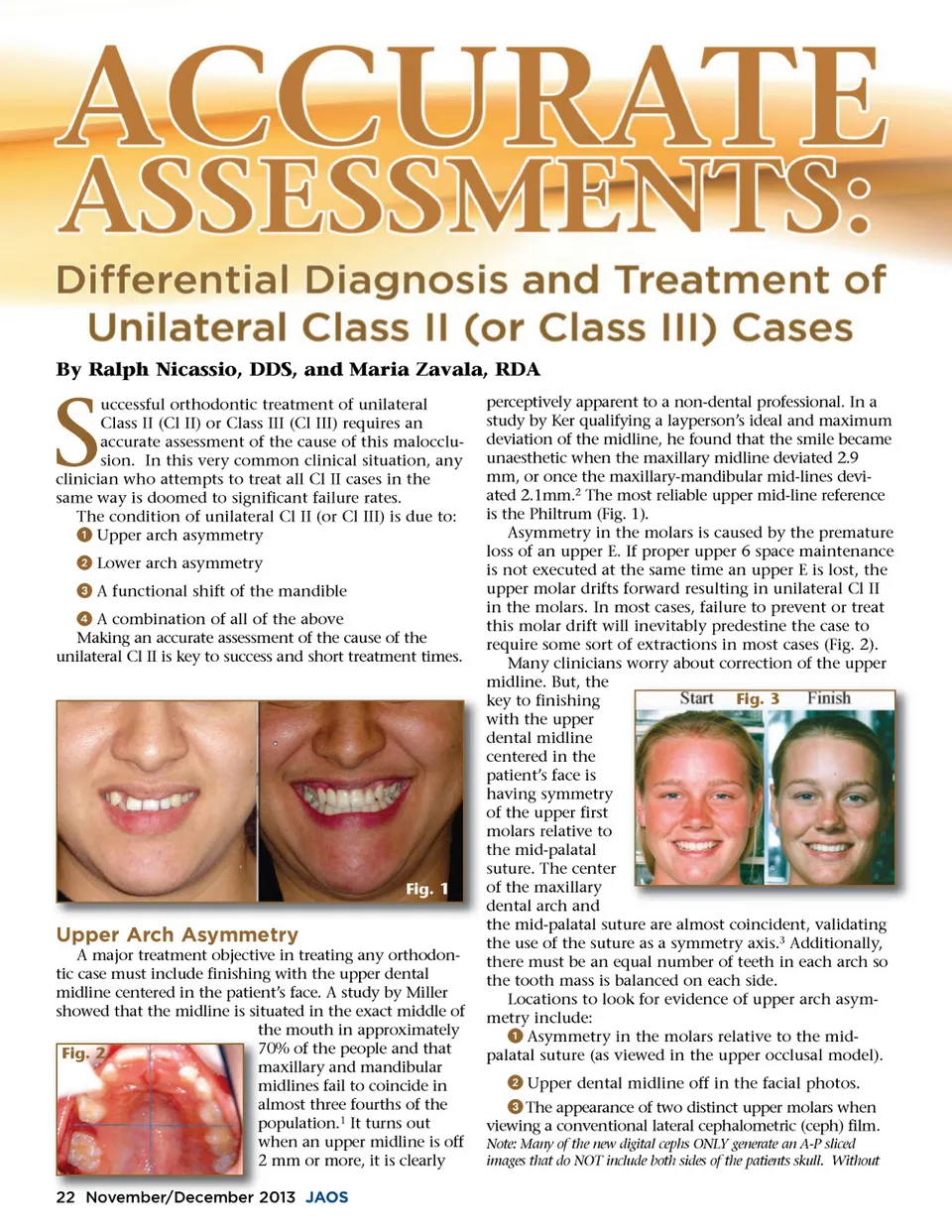
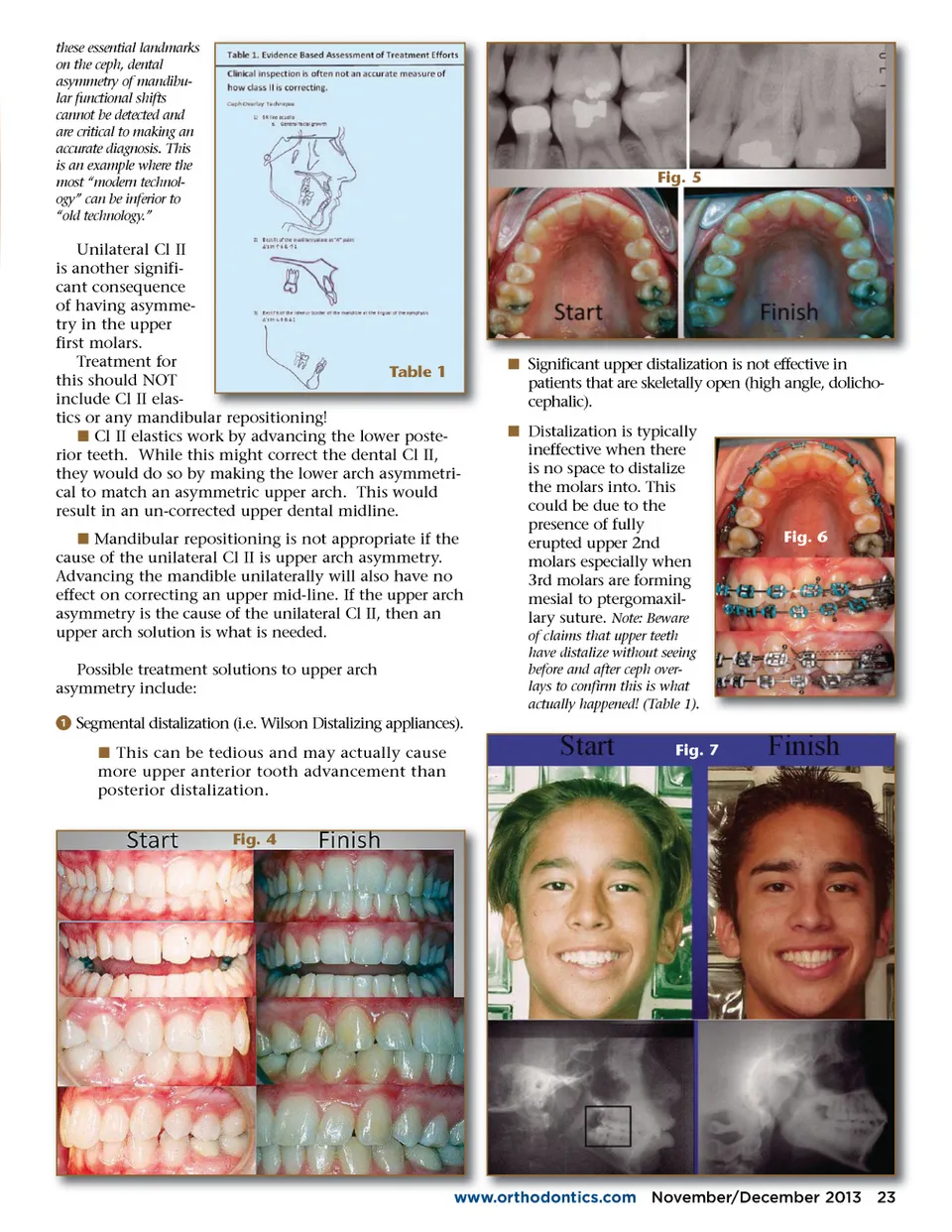
By Ralph Nicassio, DDS, and Maria Zavala, RDA S uccessful orthodontic treatment of unilateral Class II (Cl II) or Class III (Cl III) requires an accurate assessment of the cause of this malocclu-sion. In this very common clinical situation, any clinician who attempts to treat all Cl II cases in the same way is doomed to significant failure rates. The condition of unilateral Cl II (or Cl III) is due to: ᕡ Upper arch asymmetry ᕢ Lower arch asymmetry ᕣ A functional shift of the mandible ᕤ A combination of all of the above Making an accurate assessment of the cause of the unilateral Cl II is key to success and short treatment times. Fig. 1 Upper Arch Asymmetry A major treatment objective in treating any orthodon-tic case must include finishing with the upper dental midline centered in the patient’s face. A study by Miller showed that the midline is situated in the exact middle of the mouth in approximately 7 70% of the people and that Fig. 2 m maxillary and mandibular midlines fail to coincide in m almost three fourths of the a population. 1 It turns out p when w an upper midline is off 2 mm or more, it is clearly 22 November/December November/ r December 2013 2 JAOS perceptively apparent to a non-dental professional. In a study by Ker qualifying a layperson’s ideal and maximum deviation of the midline, he found that the smile became unaesthetic when the maxillary midline deviated 2.9 mm, or once the maxillary-mandibular mid-lines devi-ated 2.1mm. 2 The most reliable upper mid-line reference is the Philtrum (Fig. 1). Asymmetry in the molars is caused by the premature loss of an upper E. If proper upper 6 space maintenance is not executed at the same time an upper E is lost, the upper molar drifts forward resulting in unilateral Cl II in the molars. In most cases, failure to prevent or treat this molar drift will inevitably predestine the case to require some sort of extractions in most cases (Fig. 2). Many clinicians worry about correction of the upper midline. But, the Fig. 3 key to finishing with the upper dental midline centered in the patient’s face is having symmetry of the upper first molars relative to the mid-palatal suture. The center of the maxillary dental arch and the mid-palatal suture are almost coincident, validating the use of the suture as a symmetry axis. 3 Additionally, there must be an equal number of teeth in each arch so the tooth mass is balanced on each side. Locations to look for evidence of upper arch asym-metry include: ᕡ Asymmetry in the molars relative to the mid-palatal suture (as viewed in the upper occlusal model). ᕢ Upper dental midline off in the facial photos. ᕣ The appearance of two distinct upper molars when viewing a conventional lateral cephalometric (ceph) film. Note: Many of the new digital cephs ONLY generate an A-P sliced images that do NOT include both sides of the patients skull. Without
Journal of the American Orthodontic Society November-December 2013: Page 22