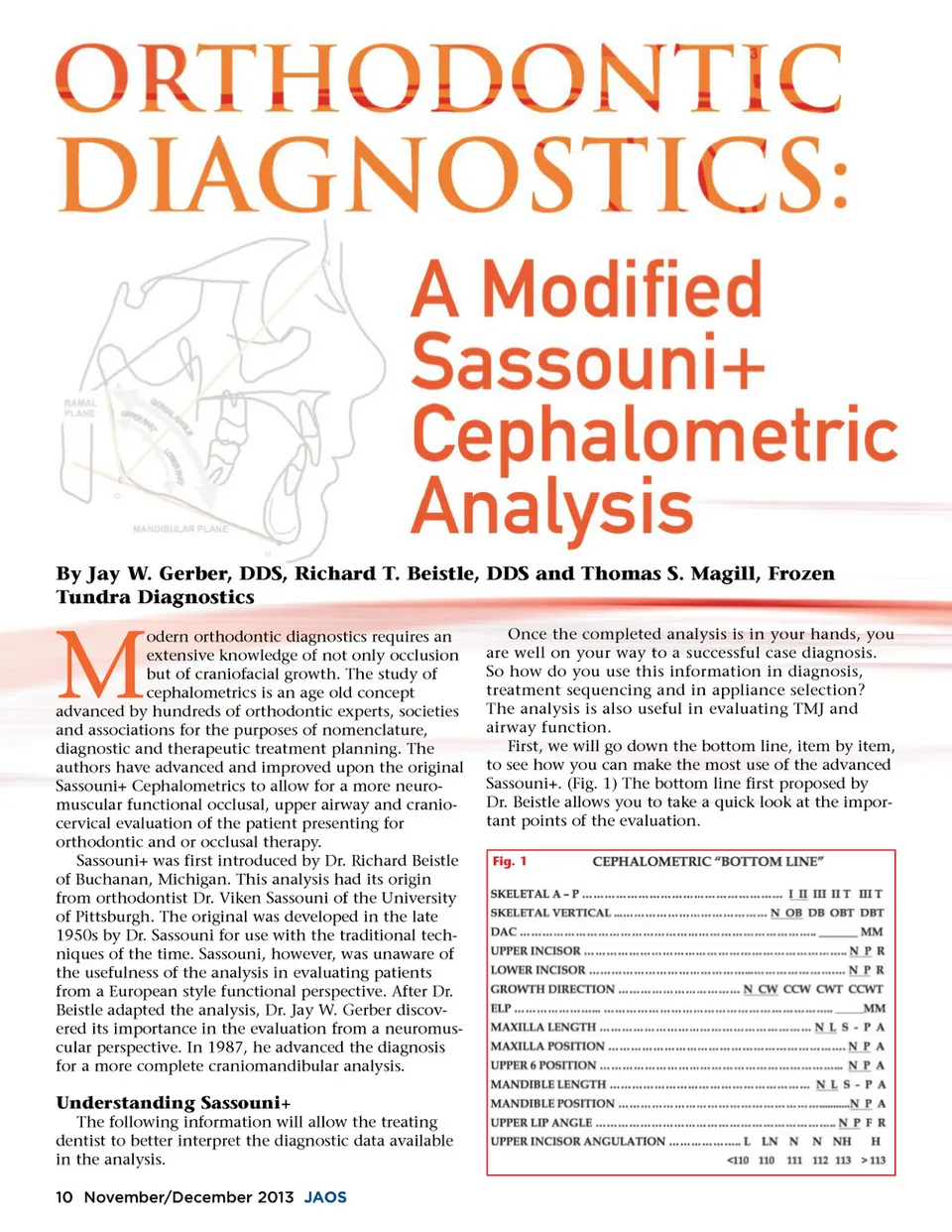
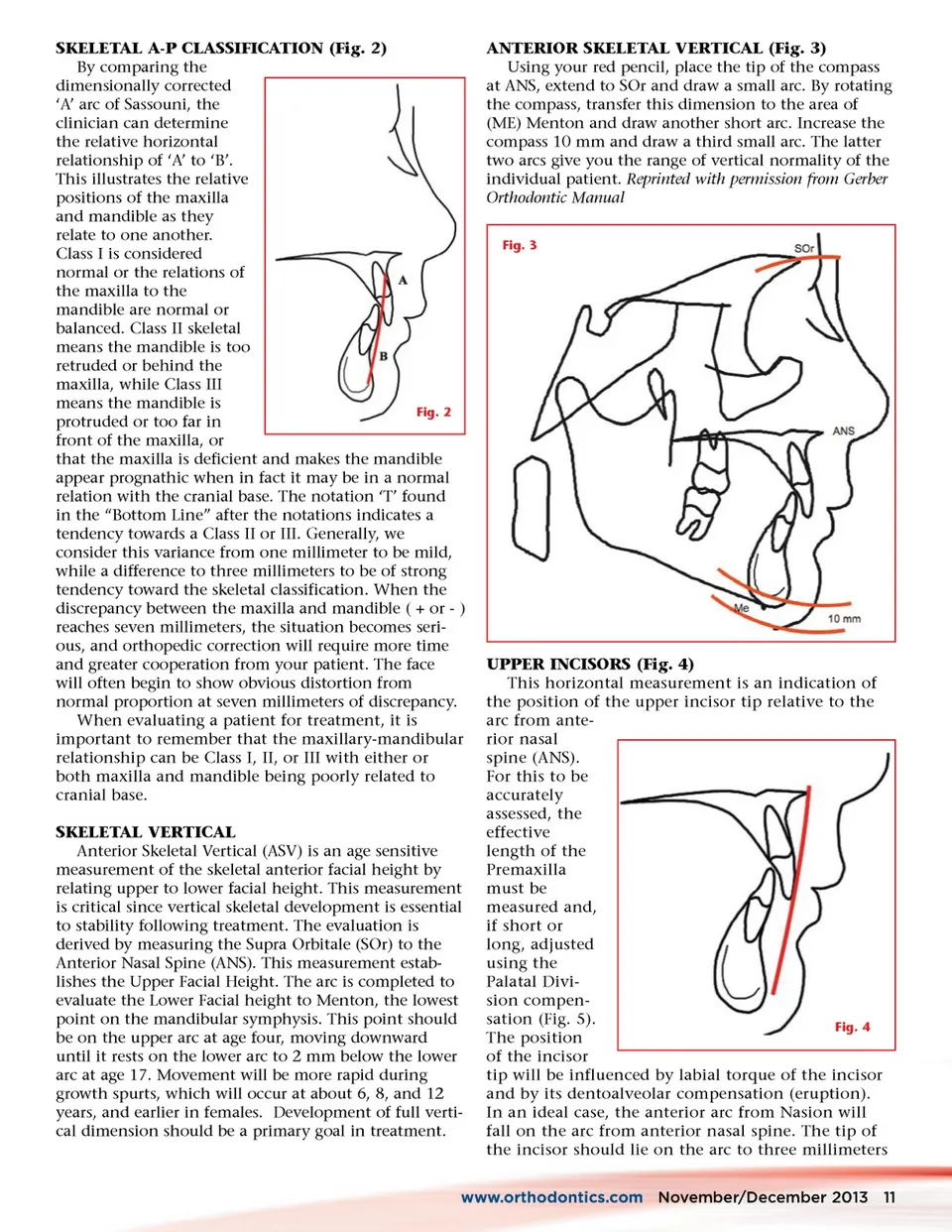
SKELETAL A-P CLASSIFICATION (Fig. 2) By comparing the dimensionally corrected ‘A’ arc of Sassouni, the clinician can determine the relative horizontal relationship of ‘A’ to ‘B’. This illustrates the relative positions of the maxilla and mandible as they relate to one another. Class I is considered normal or the relations of the maxilla to the mandible are normal or balanced. Class II skeletal means the mandible is too retruded or behind the maxilla, while Class III means the mandible is Fig. 2 protruded or too far in front of the maxilla, or that the maxilla is deficient and makes the mandible appear prognathic when in fact it may be in a normal relation with the cranial base. The notation ‘T’ found in the “Bottom Line” after the notations indicates a tendency towards a Class II or III. Generally, we consider this variance from one millimeter to be mild, while a difference to three millimeters to be of strong tendency toward the skeletal classification. When the discrepancy between the maxilla and mandible ( + or -) reaches seven millimeters, the situation becomes seri-ous, and orthopedic correction will require more time and greater cooperation from your patient. The face will often begin to show obvious distortion from normal proportion at seven millimeters of discrepancy. When evaluating a patient for treatment, it is important to remember that the maxillary-mandibular relationship can be Class I, II, or III with either or both maxilla and mandible being poorly related to cranial base. SKELETAL VERTICAL Anterior Skeletal Vertical (ASV) is an age sensitive measurement of the skeletal anterior facial height by relating upper to lower facial height. This measurement is critical since vertical skeletal development is essential to stability following treatment. The evaluation is derived by measuring the Supra Orbitale (SOr) to the Anterior Nasal Spine (ANS). This measurement estab-lishes the Upper Facial Height. The arc is completed to evaluate the Lower Facial height to Menton, the lowest point on the mandibular symphysis. This point should be on the upper arc at age four, moving downward until it rests on the lower arc to 2 mm below the lower arc at age 17. Movement will be more rapid during growth spurts, which will occur at about 6, 8, and 12 years, and earlier in females. Development of full verti-cal dimension should be a primary goal in treatment. ANTERIOR SKELETAL VERTICAL (Fig. 3) Using your red pencil, place the tip of the compass at ANS, extend to SOr and draw a small arc. By rotating the compass, transfer this dimension to the area of (ME) Menton and draw another short arc. Increase the compass 10 mm and draw a third small arc. The latter two arcs give you the range of vertical normality of the individual patient. Reprinted with permission from Gerber Orthodontic Manual Fig. 3 UPPER INCISORS (Fig. 4) This horizontal measurement is an indication of the position of the upper incisor tip relative to the arc from ante-rior nasal spine (ANS). For this to be accurately assessed, the effective length of the Premaxilla must be measured and, if short or long, adjusted using the Palatal Divi-sion compen-sation (Fig. 5). Fig. 4 The position of the incisor tip will be influenced by labial torque of the incisor and by its dentoalveolar compensation (eruption). In an ideal case, the anterior arc from Nasion will fall on the arc from anterior nasal spine. The tip of the incisor should lie on the arc to three millimeters www.orthodontics.com November/December 2013 11
Journal of the American Orthodontic Society November-December 2013: Page 11