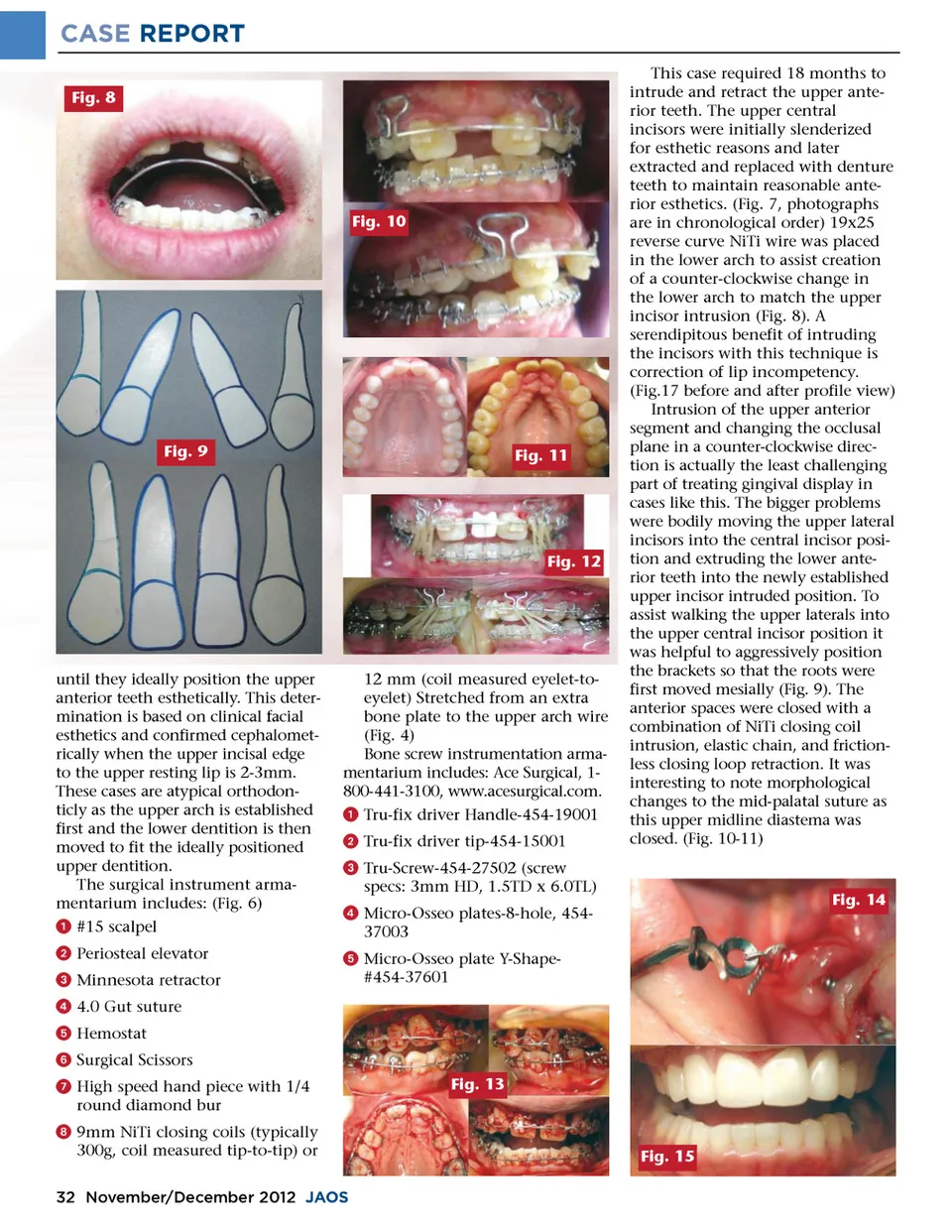
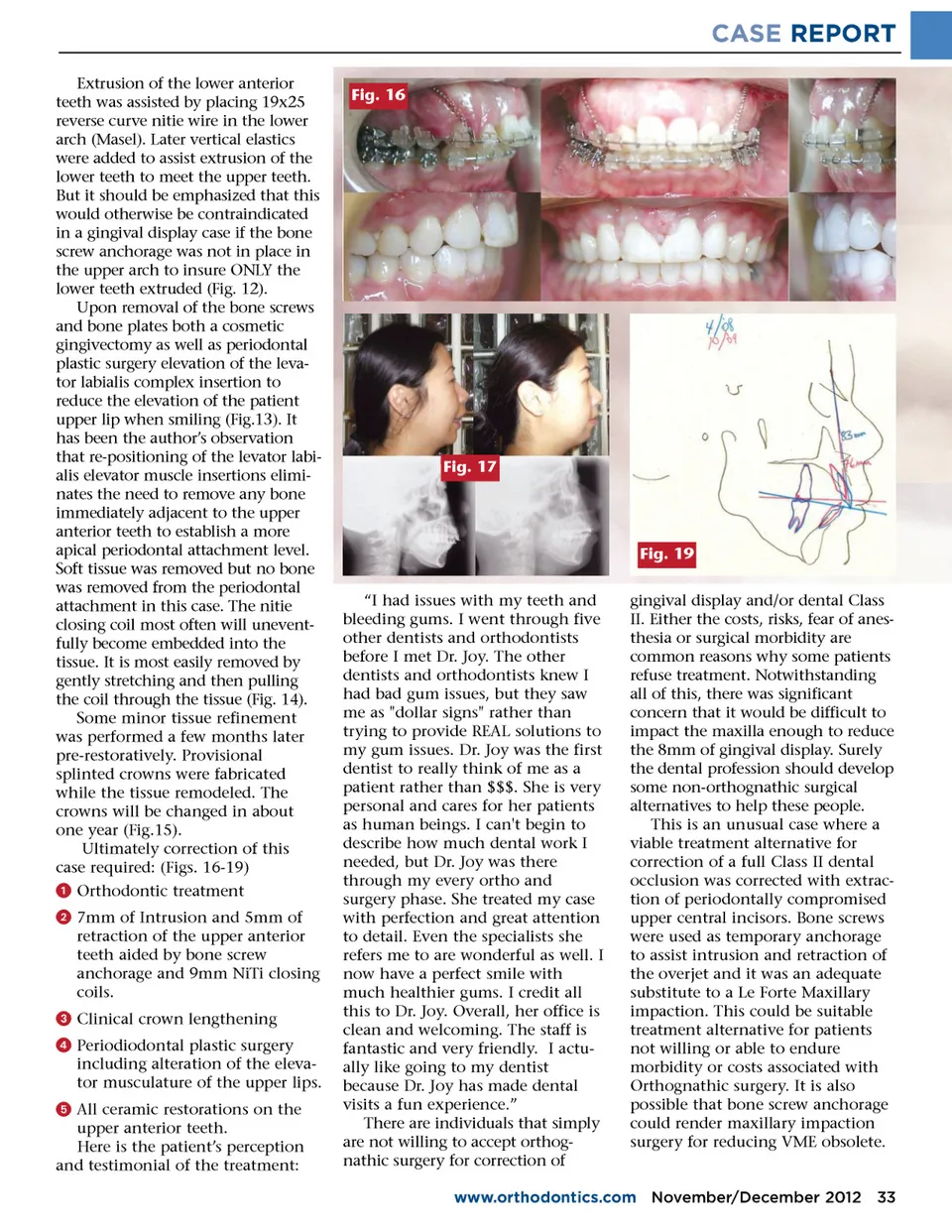
CASE REPORT Fig. 8 This case required 18 months to intrude and retract the upper ante-rior teeth. The upper central incisors were initially slenderized for esthetic reasons and later extracted and replaced with denture teeth to maintain reasonable ante-rior esthetics. (Fig. 7, photographs are in chronological order) 19x25 reverse curve NiTi wire was placed in the lower arch to assist creation of a counter-clockwise change in the lower arch to match the upper incisor intrusion (Fig. 8). A serendipitous benefit of intruding the incisors with this technique is correction of lip incompetency. (Fig.17 before and after profile view) Intrusion of the upper anterior segment and changing the occlusal plane in a counter-clockwise direc-tion is actually the least challenging part of treating gingival display in cases like this. The bigger problems were bodily moving the upper lateral incisors into the central incisor posi-tion and extruding the lower ante-rior teeth into the newly established upper incisor intruded position. To assist walking the upper laterals into the upper central incisor position it was helpful to aggressively position the brackets so that the roots were first moved mesially (Fig. 9). The anterior spaces were closed with a combination of NiTi closing coil intrusion, elastic chain, and friction-less closing loop retraction. It was interesting to note morphological changes to the mid-palatal suture as this upper midline diastema was closed. (Fig. 10-11) Fig. 10 Fig. 9 Fig. 11 Fig. 12 until they ideally position the upper anterior teeth esthetically. This deter-mination is based on clinical facial esthetics and confirmed cephalomet-rically when the upper incisal edge to the upper resting lip is 2-3mm. These cases are atypical orthodon-ticly as the upper arch is established first and the lower dentition is then moved to fit the ideally positioned upper dentition. The surgical instrument arma-mentarium includes: (Fig. 6) ᕡ #15 scalpel ᕢ Periosteal elevator ᕣ Minnesota retractor ᕤ 4.0 Gut suture ᕥ Hemostat ᕦ Surgical Scissors ᕧ High speed hand piece with 1/4 round diamond bur ᕨ 9mm NiTi closing coils (typically 300g, coil measured tip-to-tip) or 12 mm (coil measured eyelet-to-eyelet) Stretched from an extra bone plate to the upper arch wire (Fig. 4) Bone screw instrumentation arma-mentarium includes: Ace Surgical, 1-800-441-3100, www.acesurgical.com. ᕡ Tru-fix driver Handle-454-19001 ᕢ Tru-fix driver tip-454-15001 ᕣ Tru-Screw-454-27502 (screw specs: 3mm HD, 1.5TD x 6.0TL) ᕤ Micro-Osseo plates-8-hole, 454-37003 ᕥ Micro-Osseo plate Y-Shape-#454-37601 Fig. 14 Fig. 13 Fig. 15 32 November/December 2012 JAOS
Journal of the American Orthodontic Society November-December 2012: Page 32