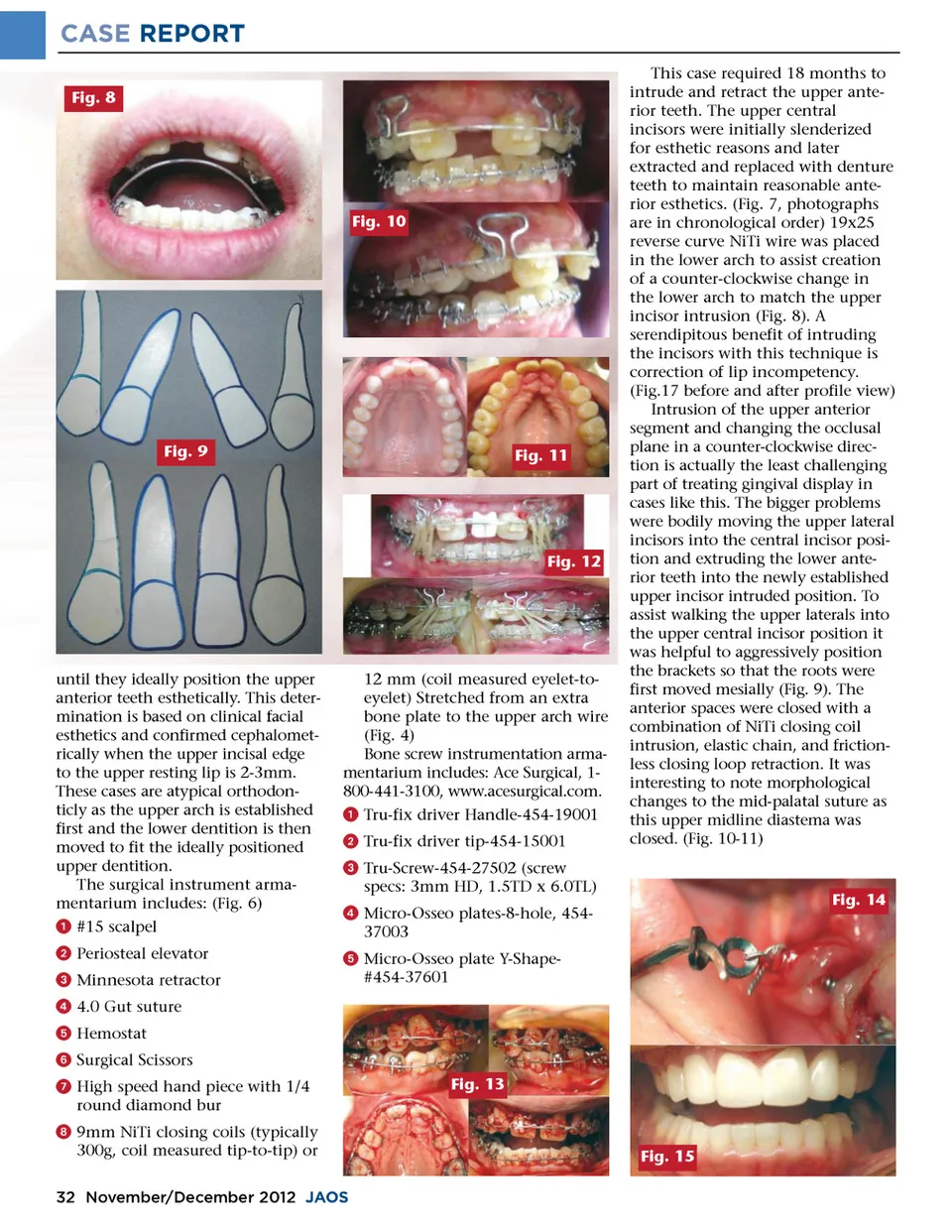
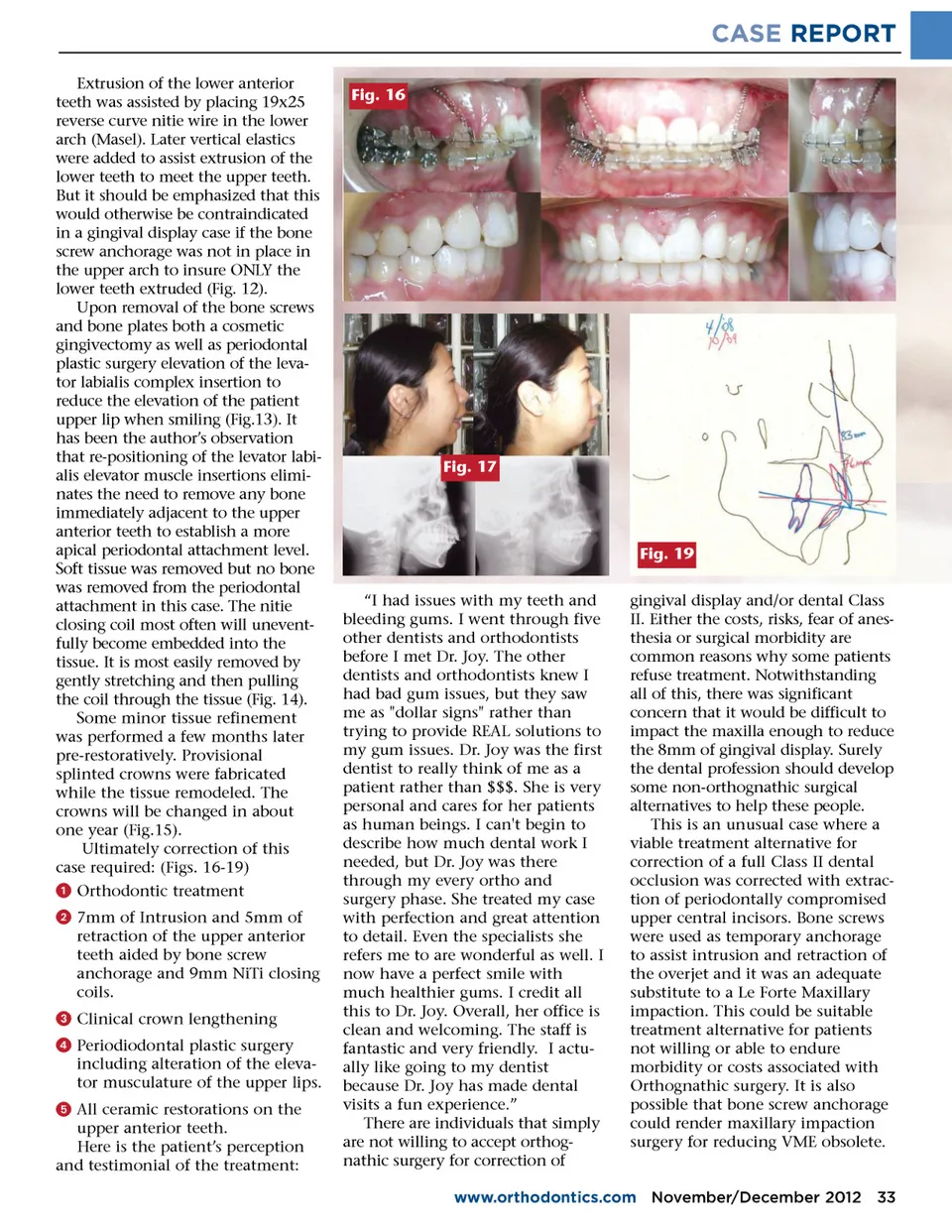
CASE REPORT Extrusion of the lower anterior teeth was assisted by placing 19x25 reverse curve nitie wire in the lower arch (Masel). Later vertical elastics were added to assist extrusion of the lower teeth to meet the upper teeth. But it should be emphasized that this would otherwise be contraindicated in a gingival display case if the bone screw anchorage was not in place in the upper arch to insure ONLY the lower teeth extruded (Fig. 12). Upon removal of the bone screws and bone plates both a cosmetic gingivectomy as well as periodontal plastic surgery elevation of the leva-tor labialis complex insertion to reduce the elevation of the patient upper lip when smiling (Fig.13). It has been the author’s observation that re-positioning of the levator labi-alis elevator muscle insertions elimi-nates the need to remove any bone immediately adjacent to the upper anterior teeth to establish a more apical periodontal attachment level. Soft tissue was removed but no bone was removed from the periodontal attachment in this case. The nitie closing coil most often will unevent-fully become embedded into the tissue. It is most easily removed by gently stretching and then pulling the coil through the tissue (Fig. 14). Some minor tissue refinement was performed a few months later pre-restoratively. Provisional splinted crowns were fabricated while the tissue remodeled. The crowns will be changed in about one year (Fig.15). Ultimately correction of this case required: (Figs. 16-19) ᕡ Orthodontic treatment ᕢ 7mm of Intrusion and 5mm of retraction of the upper anterior teeth aided by bone screw anchorage and 9mm NiTi closing coils. ᕣ Clinical crown lengthening ᕤ Periodiodontal plastic surgery including alteration of the eleva-tor musculature of the upper lips. ᕥ All ceramic restorations on the upper anterior teeth. Here is the patient’s perception and testimonial of the treatment: Fig. 16 Fig. 17 Fig. 19 “I had issues with my teeth and bleeding gums. I went through five other dentists and orthodontists before I met Dr. Joy. The other dentists and orthodontists knew I had bad gum issues, but they saw me as "dollar signs" rather than trying to provide REAL solutions to my gum issues. Dr. Joy was the first dentist to really think of me as a patient rather than $$$. She is very personal and cares for her patients as human beings. I can't begin to describe how much dental work I needed, but Dr. Joy was there through my every ortho and surgery phase. She treated my case with perfection and great attention to detail. Even the specialists she refers me to are wonderful as well. I now have a perfect smile with much healthier gums. I credit all this to Dr. Joy. Overall, her office is clean and welcoming. The staff is fantastic and very friendly. I actu-ally like going to my dentist because Dr. Joy has made dental visits a fun experience.” There are individuals that simply are not willing to accept orthog-nathic surgery for correction of gingival display and/or dental Class II. Either the costs, risks, fear of anes-thesia or surgical morbidity are common reasons why some patients refuse treatment. Notwithstanding all of this, there was significant concern that it would be difficult to impact the maxilla enough to reduce the 8mm of gingival display. Surely the dental profession should develop some non-orthognathic surgical alternatives to help these people. This is an unusual case where a viable treatment alternative for correction of a full Class II dental occlusion was corrected with extrac-tion of periodontally compromised upper central incisors. Bone screws were used as temporary anchorage to assist intrusion and retraction of the overjet and it was an adequate substitute to a Le Forte Maxillary impaction. This could be suitable treatment alternative for patients not willing or able to endure morbidity or costs associated with Orthognathic surgery. It is also possible that bone screw anchorage could render maxillary impaction surgery for reducing VME obsolete. www.orthodontics.com November/December 2012 33
Journal of the American Orthodontic Society November-December 2012: Page 33