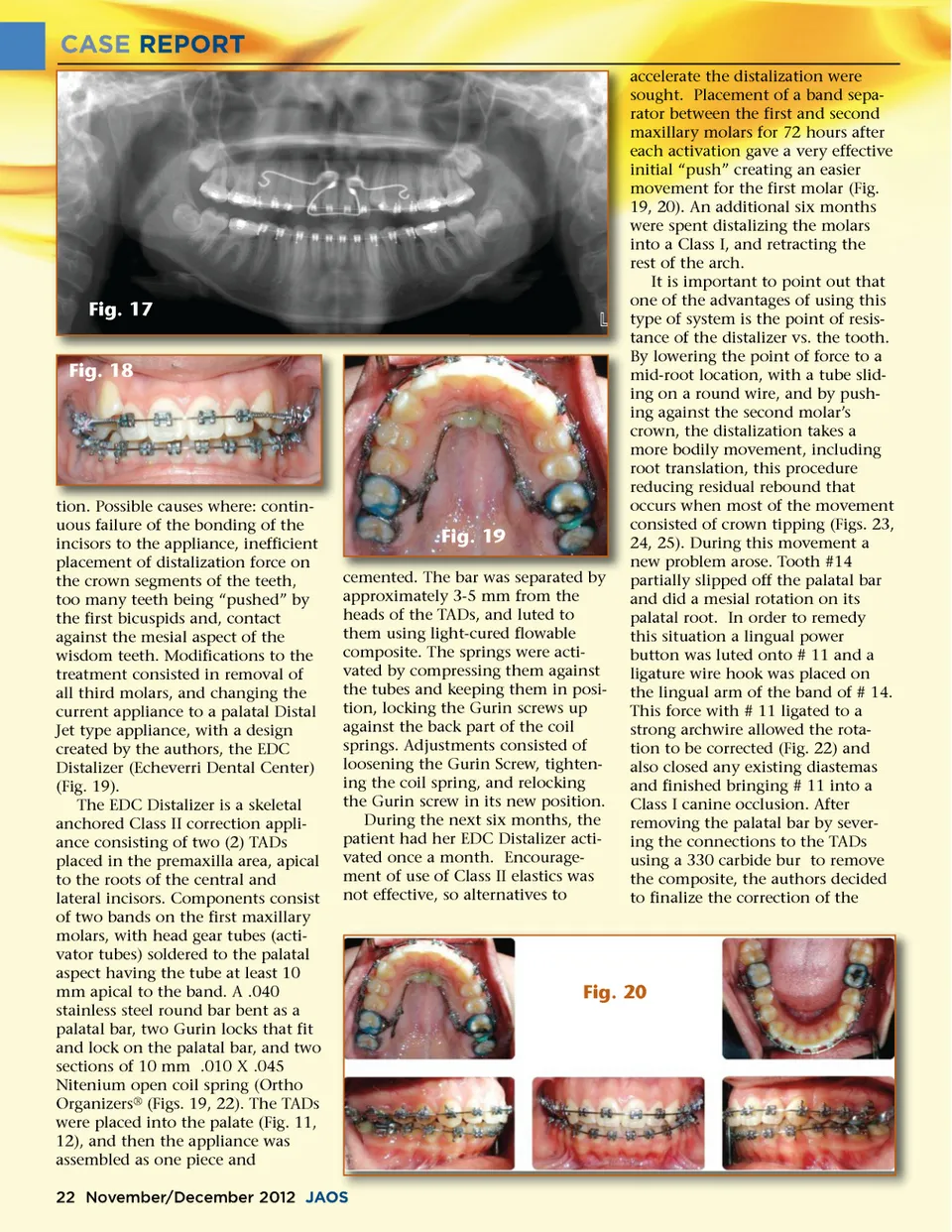
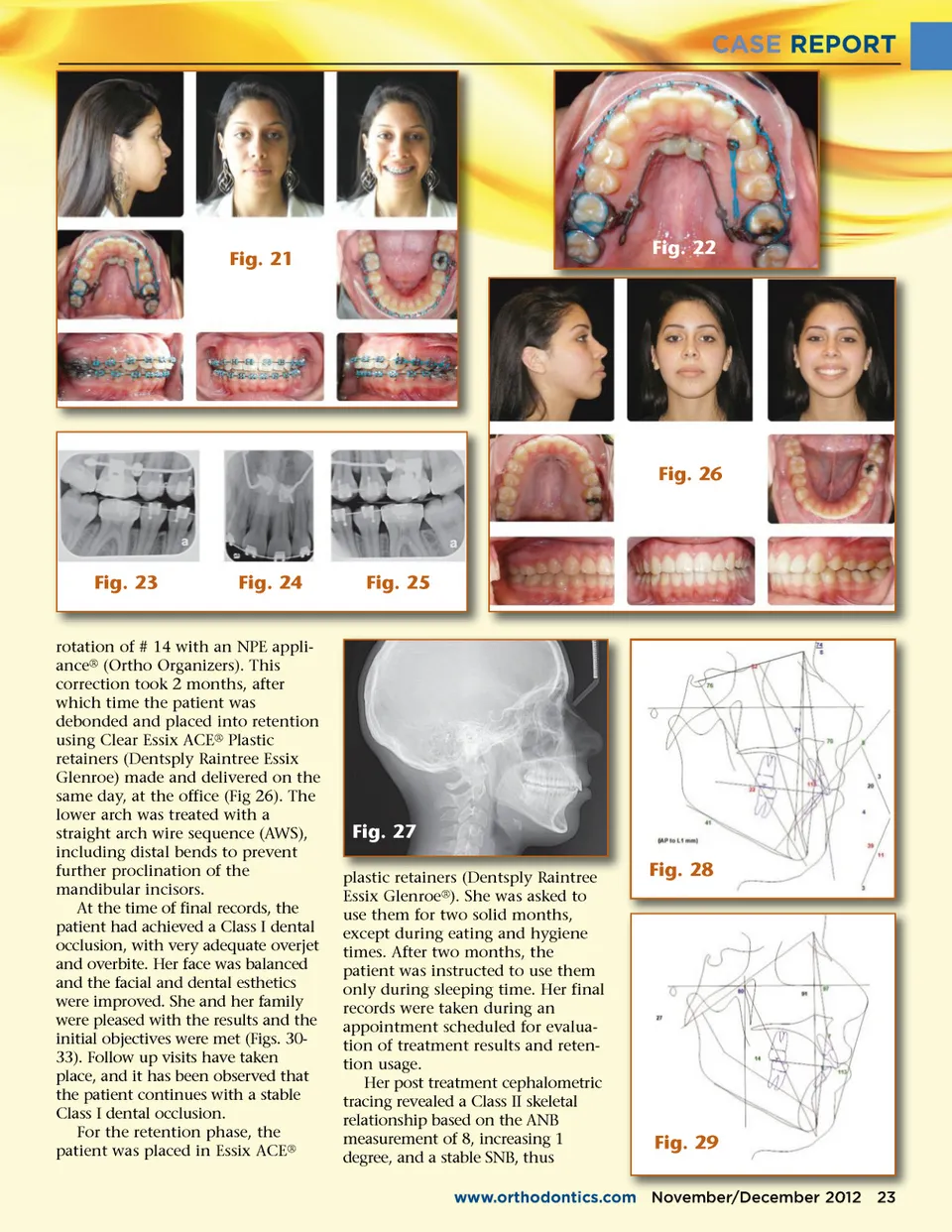
CASE REPORT accelerate the distalization were sought. Placement of a band sepa-rator between the first and second maxillary molars for 72 hours after each activation gave a very effective initial “push” creating an easier movement for the first molar (Fig. 19, 20). An additional six months were spent distalizing the molars into a Class I, and retracting the rest of the arch. It is important to point out that one of the advantages of using this type of system is the point of resis-tance of the distalizer vs. the tooth. By lowering the point of force to a mid-root location, with a tube slid-ing on a round wire, and by push-ing against the second molar’s crown, the distalization takes a more bodily movement, including root translation, this procedure reducing residual rebound that occurs when most of the movement consisted of crown tipping (Figs. 23, 24, 25). During this movement a new problem arose. Tooth #14 partially slipped off the palatal bar and did a mesial rotation on its palatal root. In order to remedy this situation a lingual power button was luted onto # 11 and a ligature wire hook was placed on the lingual arm of the band of # 14. This force with # 11 ligated to a strong archwire allowed the rota-tion to be corrected (Fig. 22) and also closed any existing diastemas and finished bringing # 11 into a Class I canine occlusion. After removing the palatal bar by sever-ing the connections to the TADs using a 330 carbide bur to remove the composite, the authors decided to finalize the correction of the Fig. 17 Fig. 18 tion Possible causes where: contin tion. contin-uous failure of the bonding of the incisors to the appliance, inefficient placement of distalization force on the crown segments of the teeth, too many teeth being “pushed” by the first bicuspids and, contact against the mesial aspect of the wisdom teeth. Modifications to the treatment consisted in removal of all third molars, and changing the current appliance to a palatal Distal Jet type appliance, with a design created by the authors, the EDC Distalizer (Echeverri Dental Center) (Fig. 19). The EDC Distalizer is a skeletal anchored Class II correction appli-ance consisting of two (2) TADs placed in the premaxilla area, apical to the roots of the central and lateral incisors. Components consist of two bands on the first maxillary molars, with head gear tubes (acti-vator tubes) soldered to the palatal aspect having the tube at least 10 mm apical to the band. A .040 stainless steel round bar bent as a palatal bar, two Gurin locks that fit and lock on the palatal bar, and two sections of 10 mm .010 X .045 Nitenium open coil spring (Ortho Organizers ® (Figs. 19, 22). The TADs were placed into the palate (Fig. 11, 12), and then the appliance was assembled as one piece and Fig. 19 cemented. cemented The bar was separated by approximately 3-5 mm from the heads of the TADs, and luted to them using light-cured flowable composite. The springs were acti-vated by compressing them against the tubes and keeping them in posi-tion, locking the Gurin screws up against the back part of the coil springs. Adjustments consisted of loosening the Gurin Screw, tighten-ing the coil spring, and relocking the Gurin screw in its new position. During the next six months, the patient had her EDC Distalizer acti-vated once a month. Encourage-ment of use of Class II elastics was not effective, so alternatives to Fig. 20 22 November/December 2012 JAOS
Journal of the American Orthodontic Society November-December 2012: Page 22