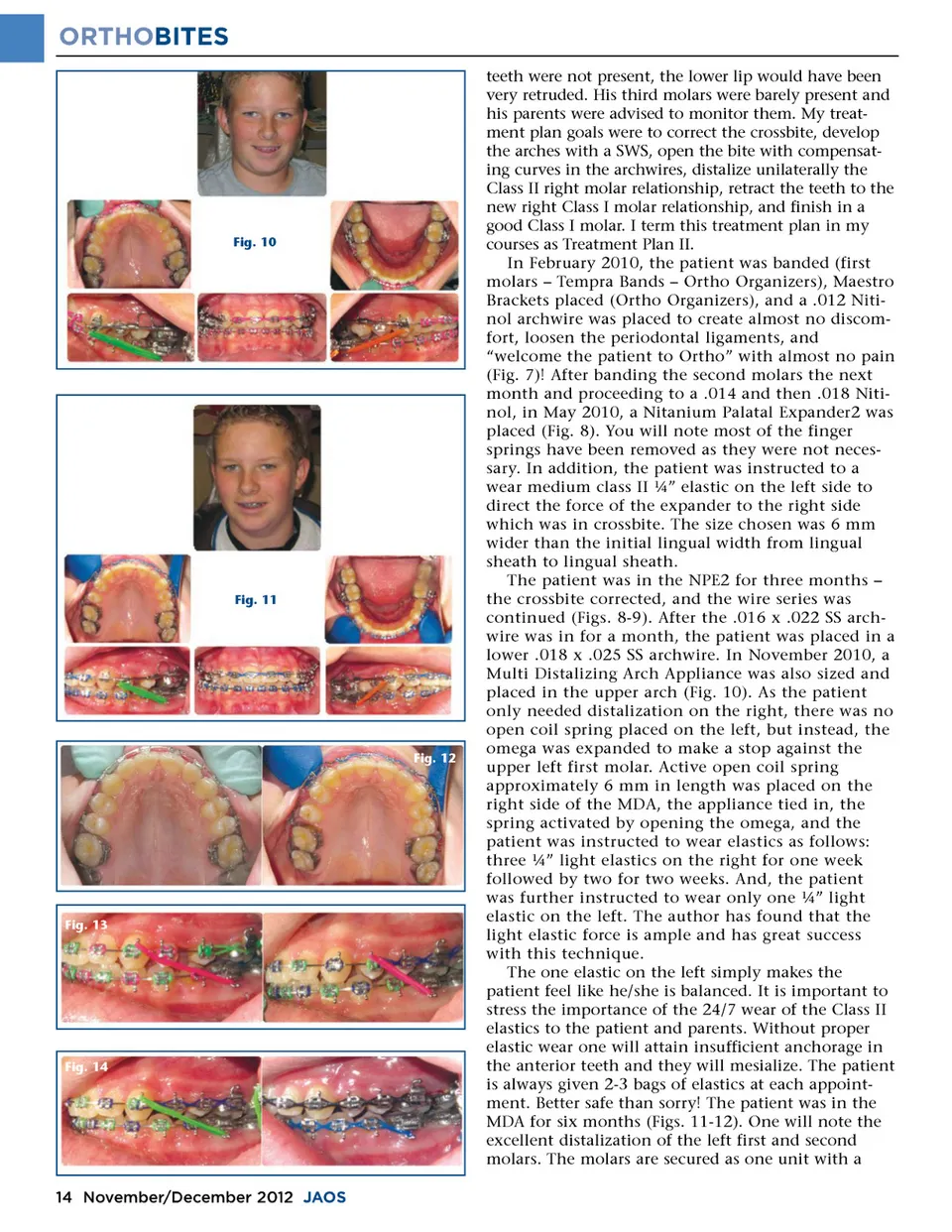
ORTHOBITES teeth were not present, the lower lip would have been very retruded. His third molars were barely present and his parents were advised to monitor them. My treat-ment plan goals were to correct the crossbite, develop the arches with a SWS, open the bite with compensat-ing curves in the archwires, distalize unilaterally the Class II right molar relationship, retract the teeth to the new right Class I molar relationship, and finish in a good Class I molar. I term this treatment plan in my courses as Treatment Plan II. In February 2010, the patient was banded (first molars – Tempra Bands – Ortho Organizers), Maestro Brackets placed (Ortho Organizers), and a .012 Niti-nol archwire was placed to create almost no discom-fort, loosen the periodontal ligaments, and “welcome the patient to Ortho” with almost no pain (Fig. 7)! After banding the second molars the next month and proceeding to a .014 and then .018 Niti-nol, in May 2010, a Nitanium Palatal Expander2 was placed (Fig. 8). You will note most of the finger springs have been removed as they were not neces-sary. In addition, the patient was instructed to a wear medium class II ¼” elastic on the left side to direct the force of the expander to the right side which was in crossbite. The size chosen was 6 mm wider than the initial lingual width from lingual sheath to lingual sheath. The patient was in the NPE2 for three months – the crossbite corrected, and the wire series was continued (Figs. 8-9). After the .016 x .022 SS arch-wire was in for a month, the patient was placed in a lower .018 x .025 SS archwire. In November 2010, a Multi Distalizing Arch Appliance was also sized and placed in the upper arch (Fig. 10). As the patient only needed distalization on the right, there was no open coil spring placed on the left, but instead, the omega was expanded to make a stop against the upper left first molar. Active open coil spring approximately 6 mm in length was placed on the right side of the MDA, the appliance tied in, the spring activated by opening the omega, and the patient was instructed to wear elastics as follows: three ¼” light elastics on the right for one week followed by two for two weeks. And, the patient was further instructed to wear only one ¼” light elastic on the left. The author has found that the light elastic force is ample and has great success with this technique. The one elastic on the left simply makes the patient feel like he/she is balanced. It is important to stress the importance of the 24/7 wear of the Class II elastics to the patient and parents. Without proper elastic wear one will attain insufficient anchorage in the anterior teeth and they will mesialize. The patient is always given 2-3 bags of elastics at each appoint-ment. Better safe than sorry! The patient was in the MDA for six months (Figs. 11-12). One will note the excellent distalization of the left first and second molars. The molars are secured as one unit with a Fig. 10 Fig. 11 Fig. 12 Fig. 13 Fig. 14 14 November/December 2012 JAOS
Journal of the American Orthodontic Society November-December 2012: Page 14