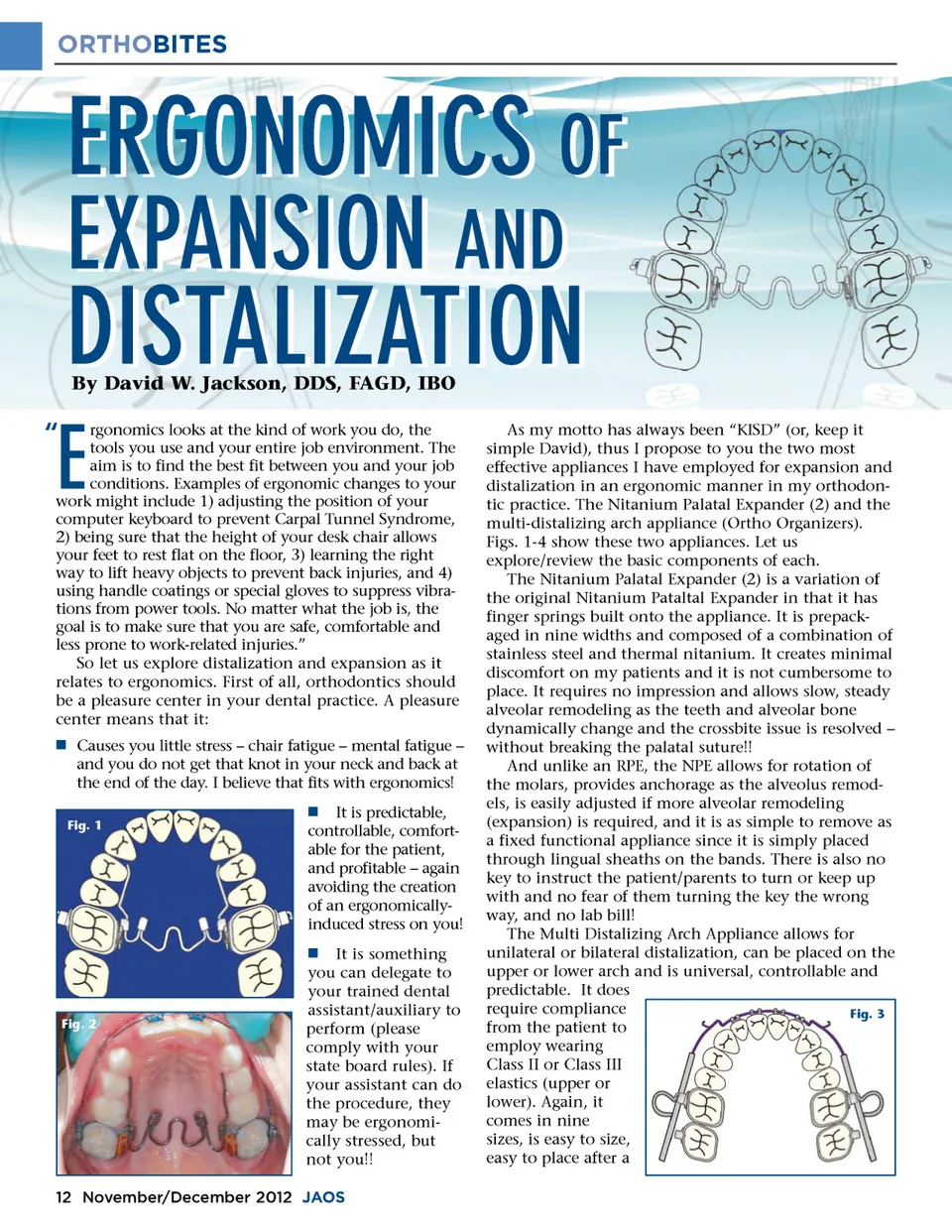
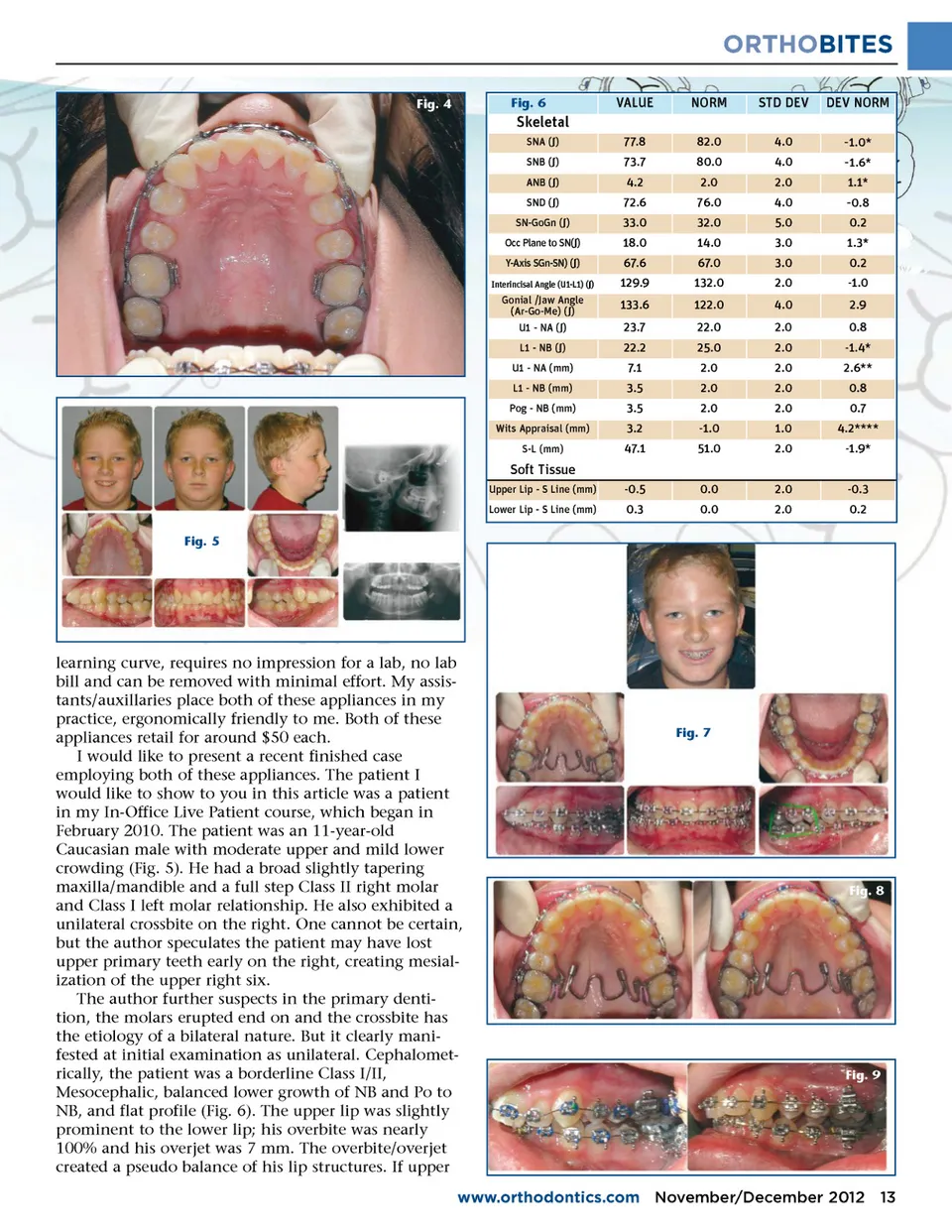
ORTHOBITES Fig. 4 Fig. 6 VALUE 77.8 73.7 4.2 72.6 33.0 18.0 67.6 129.9 133.6 23.7 22.2 7.1 3.5 3.5 3.2 47.1 -0.5 0.3 NORM 82.0 80.0 2.0 76.0 32.0 14.0 67.0 132.0 122.0 22.0 25.0 2.0 2.0 2.0 -1.0 51.0 0.0 0.0 STD DEV 4.0 4.0 2.0 4.0 5.0 3.0 3.0 2.0 4.0 2.0 2.0 2.0 2.0 2.0 1.0 2.0 2.0 2.0 DEV NORM -1.0* -1.6* 1.1* Skeletal SNA ( ∫ ) SNB ( ∫ ) ANB ( ∫ ) SND ( ∫ ) SN-GoGn ( ∫ ) Occ Plane to SN( ∫ ) Y-Axis SGn-SN) ( ∫ ) Interincisal Angle (U1-L1) ( ∫ ) -0.8 0.2 1.3* 0.2 -1.0 2.9 0.8 -1.4* 2.6** 0.8 0.7 4.2**** -1.9* -0.3 0.2 Gonial /Jaw Angle (Ar-Go-Me) ( ∫ ) U1 -NA ( ∫ ) L1 -NB ( ∫ ) U1 -NA (mm) L1 -NB (mm) Pog -NB (mm) Wits Appraisal (mm) S-L (mm) Soft Tissue Upper Lip -S Line (mm) Lower Lip -S Line (mm) Fig. 5 learning curve, requires no impression for a lab, no lab bill and can be removed with minimal effort. My assis-tants/auxillaries place both of these appliances in my practice, ergonomically friendly to me. Both of these appliances retail for around $50 each. I would like to present a recent finished case employing both of these appliances. The patient I would like to show to you in this article was a patient in my In-Office Live Patient course, which began in February 2010. The patient was an 11-year-old Caucasian male with moderate upper and mild lower crowding (Fig. 5). He had a broad slightly tapering maxilla/mandible and a full step Class II right molar and Class I left molar relationship. He also exhibited a unilateral crossbite on the right. One cannot be certain, but the author speculates the patient may have lost upper primary teeth early on the right, creating mesial-ization of the upper right six. The author further suspects in the primary denti-tion, the molars erupted end on and the crossbite has the etiology of a bilateral nature. But it clearly mani-fested at initial examination as unilateral. Cephalomet-rically, the patient was a borderline Class I/II, Mesocephalic, balanced lower growth of NB and Po to NB, and flat profile (Fig. 6). The upper lip was slightly prominent to the lower lip; his overbite was nearly 100% and his overjet was 7 mm. The overbite/overjet created a pseudo balance of his lip structures. If upper Fig. 7 Fig. 8 Fig. 9 www.orthodontics.com November/December 2012 13
Journal of the American Orthodontic Society November-December 2012: Page 13