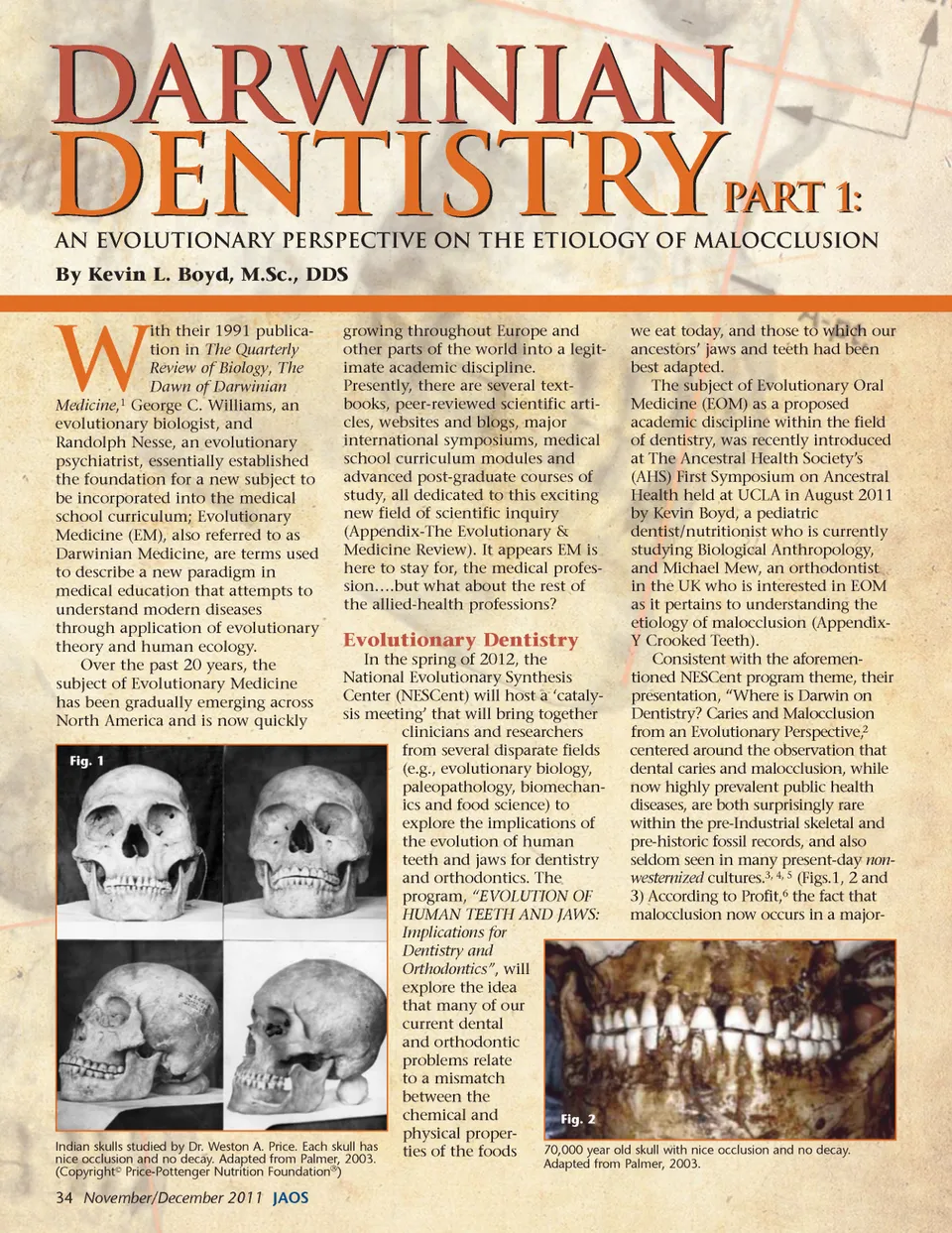
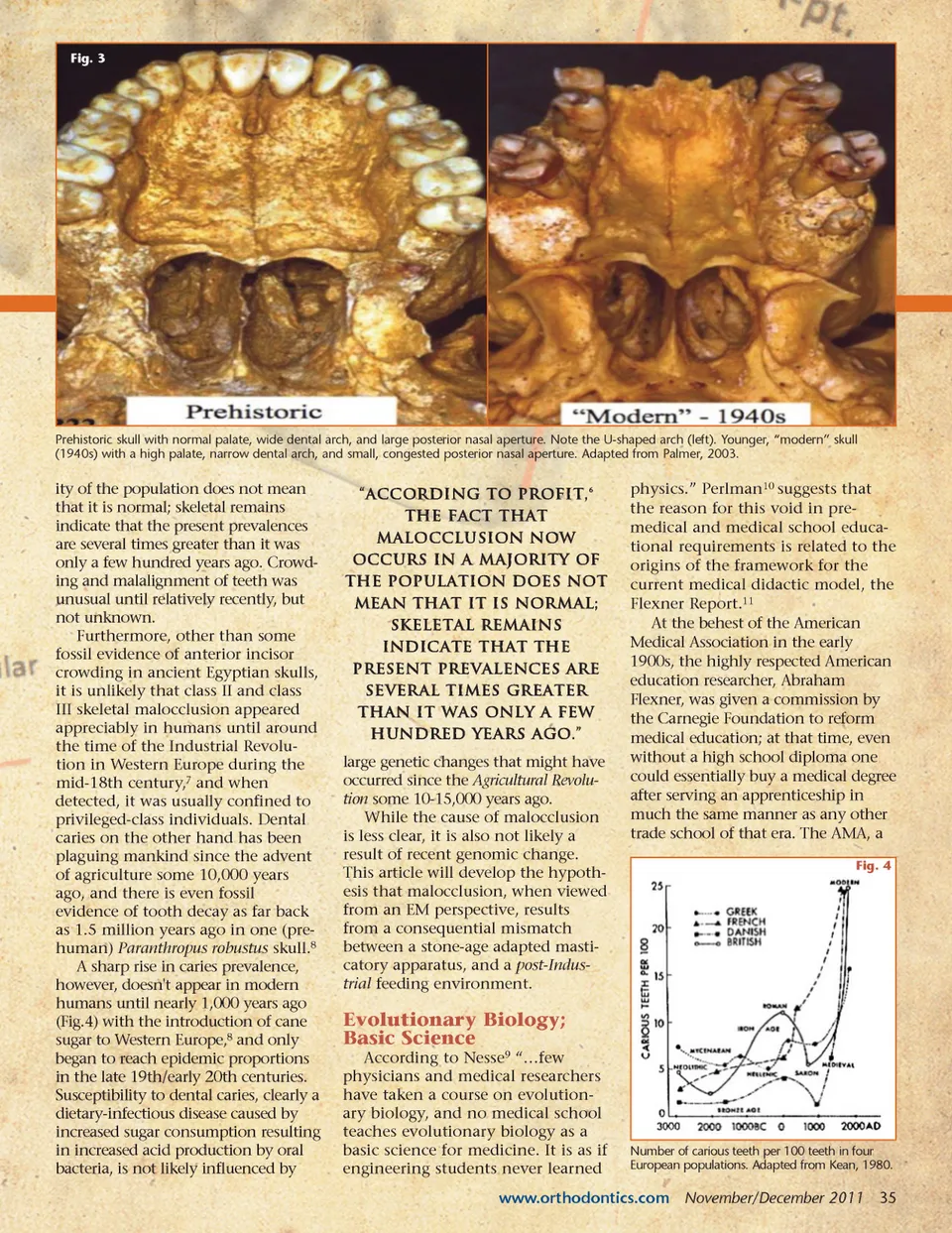
Fig. 3 Prehistoric skull with normal palate, wide dental arch, and large posterior nasal aperture. Note the U-shaped arch (left). Younger, “modern” skull (1940s) with a high palate, narrow dental arch, and small, congested posterior nasal aperture. Adapted from Palmer, 2003. ity of the population does not mean that it is normal; skeletal remains indicate that the present prevalences are several times greater than it was only a few hundred years ago. Crowd-ing and malalignment of teeth was unusual until relatively recently, but not unknown. Furthermore, other than some fossil evidence of anterior incisor crowding in ancient Egyptian skulls, it is unlikely that class II and class III skeletal malocclusion appeared appreciably in humans until around the time of the Industrial Revolu-tion in Western Europe during the mid-18th century, 7 and when detected, it was usually confined to privileged-class individuals. Dental caries on the other hand has been plaguing mankind since the advent of agriculture some 10,000 years ago, and there is even fossil evidence of tooth decay as far back as 1.5 million years ago in one (pre-human) Paranthropus robustus skull. 8 A sharp rise in caries prevalence, however, doesn't appear in modern humans until nearly 1,000 years ago (Fig.4) with the introduction of cane sugar to Western Europe, 8 and only began to reach epidemic proportions in the late 19th/early 20th centuries. Susceptibility to dental caries, clearly a dietary-infectious disease caused by increased sugar consumption resulting in increased acid production by oral bacteria, is not likely influenced by “According to Profit, 6 the fact that malocclusion now occurs in a majority of the population does not mean that it is normal; skeletal remains indicate that the present prevalences are several times greater than it was only a few hundred years ago.” large genetic changes that might have occurred since the Agricultural Revolu-tion some 10-15,000 years ago. While the cause of malocclusion is less clear, it is also not likely a result of recent genomic change. This article will develop the hypoth-esis that malocclusion, when viewed from an EM perspective, results from a consequential mismatch between a stone-age adapted masti-catory apparatus, and a post-Indus-trial feeding environment. physics.” Perlman 10 suggests that the reason for this void in pre-medical and medical school educa-tional requirements is related to the origins of the framework for the current medical didactic model, the Flexner Report. 11 At the behest of the American Medical Association in the early 1900s, the highly respected American education researcher, Abraham Flexner, was given a commission by the Carnegie Foundation to reform medical education; at that time, even without a high school diploma one could essentially buy a medical degree after serving an apprenticeship in much the same manner as any other trade school of that era. The AMA, a Fig. 4 Evolutionary Biology; Basic Science According to Nesse 9 “…few physicians and medical researchers have taken a course on evolution-ary biology, and no medical school teaches evolutionary biology as a basic science for medicine. It is as if engineering students never learned Number of carious teeth per 100 teeth in four European populations. Adapted from Kean, 1980. www.orthodontics.com November/December 2011 35
Journal of the American Orthodontic Society November-December 2011: Page 35