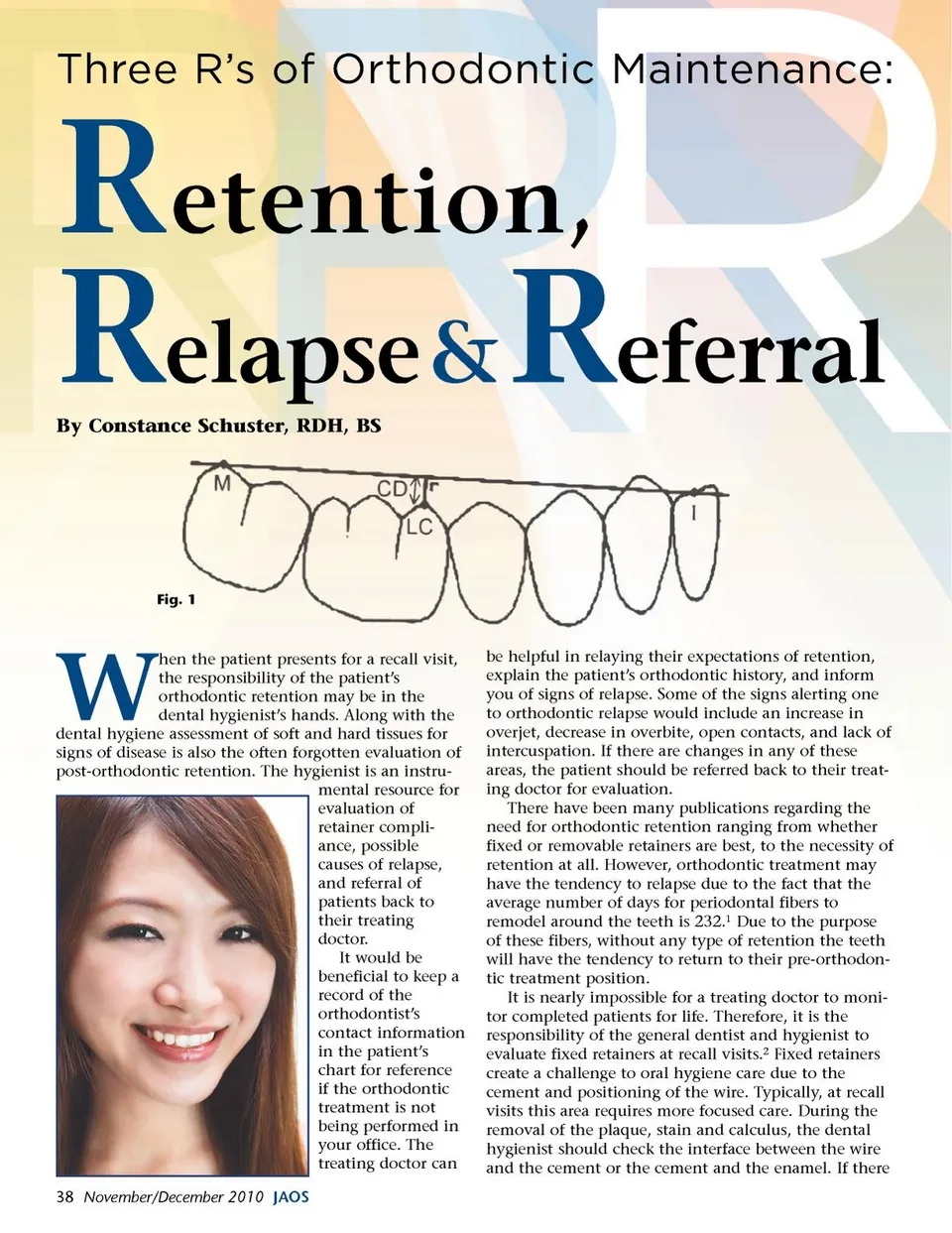
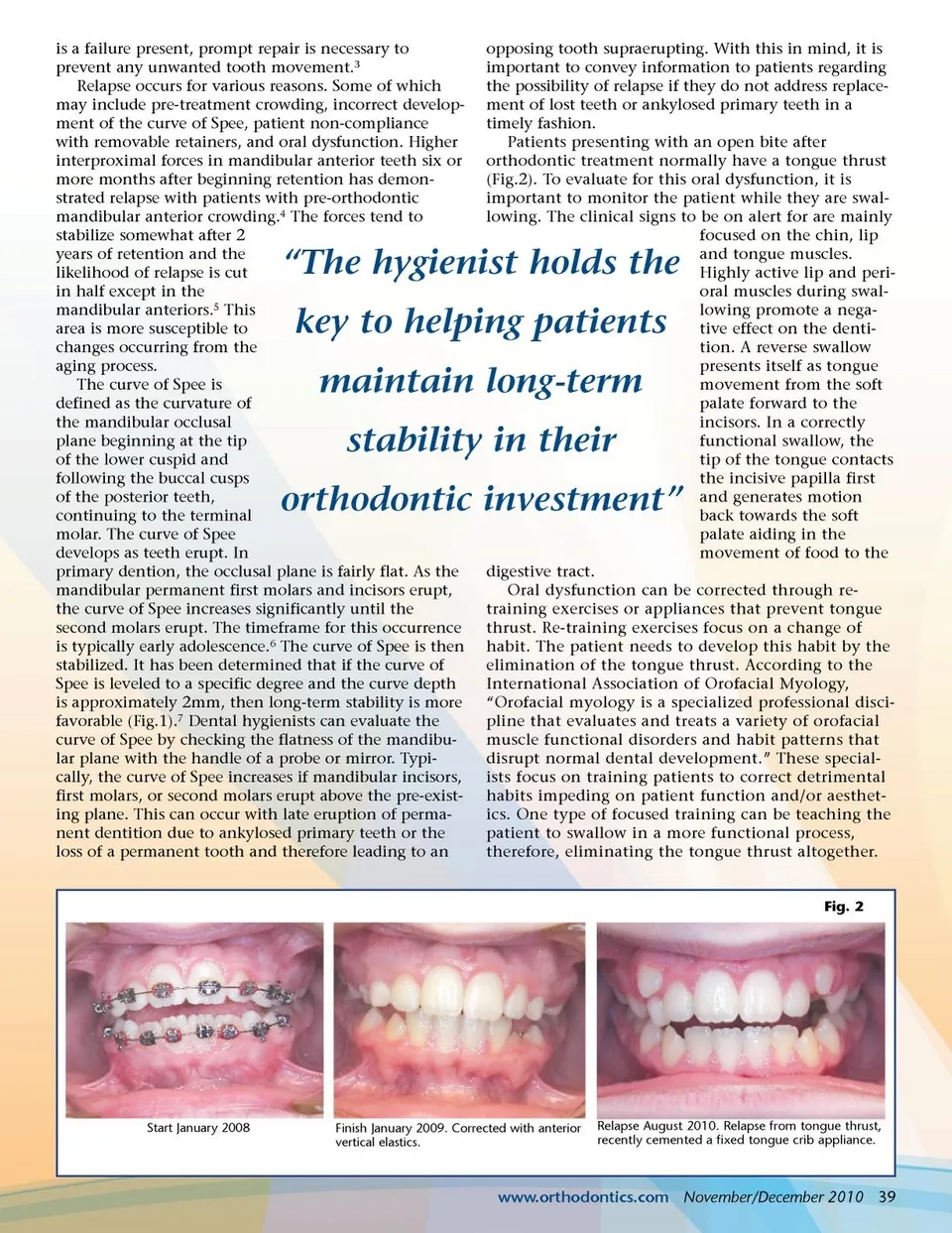
is a failure present, prompt repair is necessary to prevent any unwanted tooth movement. 3 Relapse occurs for various reasons. Some of which may include pre-treatment crowding, incorrect develop-ment of the curve of Spee, patient non-compliance with removable retainers, and oral dysfunction. Higher interproximal forces in mandibular anterior teeth six or more months after beginning retention has demon-strated relapse with patients with pre-orthodontic mandibular anterior crowding. 4 The forces tend to stabilize somewhat after 2 years of retention and the likelihood of relapse is cut in half except in the mandibular anteriors. 5 This area is more susceptible to changes occurring from the aging process. The curve of Spee is defined as the curvature of the mandibular occlusal plane beginning at the tip of the lower cuspid and following the buccal cusps of the posterior teeth, continuing to the terminal molar. The curve of Spee develops as teeth erupt. In primary dention, the occlusal plane is fairly flat. As the mandibular permanent first molars and incisors erupt, the curve of Spee increases significantly until the second molars erupt. The timeframe for this occurrence is typically early adolescence. 6 The curve of Spee is then stabilized. It has been determined that if the curve of Spee is leveled to a specific degree and the curve depth is approximately 2mm, then long-term stability is more favorable (Fig.1). 7 Dental hygienists can evaluate the curve of Spee by checking the flatness of the mandibu-lar plane with the handle of a probe or mirror. Typi-cally, the curve of Spee increases if mandibular incisors, first molars, or second molars erupt above the pre-exist-ing plane. This can occur with late eruption of perma-nent dentition due to ankylosed primary teeth or the loss of a permanent tooth and therefore leading to an “The hygienist holds the key to helping patients maintain long-term stability in their orthodontic investment” opposing tooth supraerupting. With this in mind, it is important to convey information to patients regarding the possibility of relapse if they do not address replace-ment of lost teeth or ankylosed primary teeth in a timely fashion. Patients presenting with an open bite after orthodontic treatment normally have a tongue thrust (Fig.2). To evaluate for this oral dysfunction, it is important to monitor the patient while they are swal-lowing. The clinical signs to be on alert for are mainly focused on the chin, lip and tongue muscles. Highly active lip and peri-oral muscles during swal-lowing promote a nega-tive effect on the denti-tion. A reverse swallow presents itself as tongue movement from the soft palate forward to the incisors. In a correctly functional swallow, the tip of the tongue contacts the incisive papilla first and generates motion back towards the soft palate aiding in the movement of food to the digestive tract. Oral dysfunction can be corrected through re-training exercises or appliances that prevent tongue thrust. Re-training exercises focus on a change of habit. The patient needs to develop this habit by the elimination of the tongue thrust. According to the International Association of Orofacial Myology, “Orofacial myology is a specialized professional disci-pline that evaluates and treats a variety of orofacial muscle functional disorders and habit patterns that disrupt normal dental development.” These special-ists focus on training patients to correct detrimental habits impeding on patient function and/or aesthet-ics. One type of focused training can be teaching the patient to swallow in a more functional process, therefore, eliminating the tongue thrust altogether. Fig. 2 Start January 2008 Finish January 2009. Corrected with anterior vertical elastics. Relapse August 2010. Relapse from tongue thrust, recently cemented a fixed tongue crib appliance. www.orthodontics.com November/December 2010 39
Journal of the American Orthodontic Society November-December 2010: Page 39