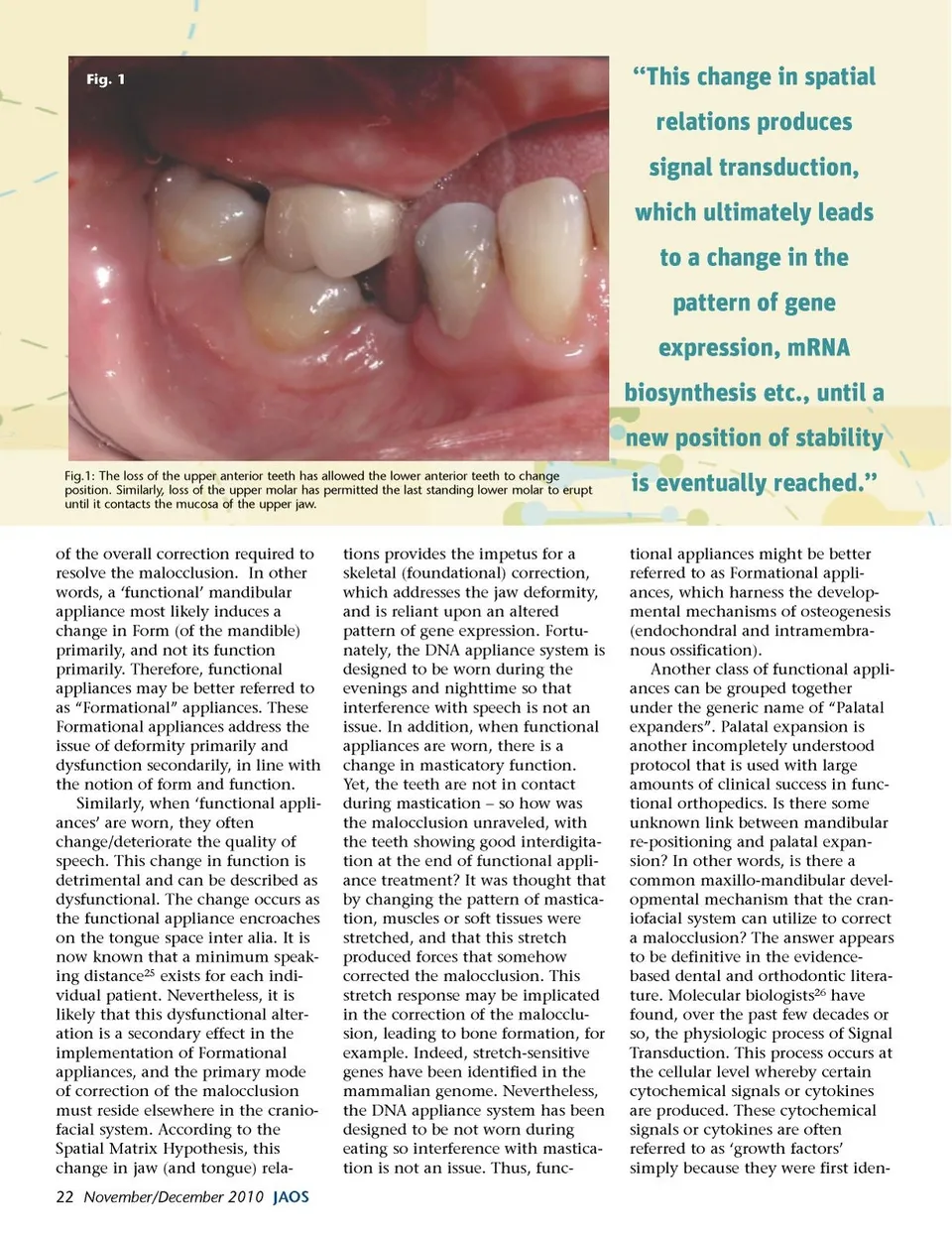
tified in embryos. (These growth factors often have effects other than growth and development alone.) Nevertheless, when a specific growth factor, such as Bone Morphogenetic Protein (BMP) attaches to its specific Receptor on the cell surface, signal transduction occurs and produces a second messenger inside the cell’s cyto-plasm. This second messenger effect is often associated with a rise in the level of cAMP in the cell. Within the cell cytoplasm, a cascade of events is initiated. Molecules that are activated in the cytoplasm translocate into the cell’s nucleus. Here they form complexes with nuclear co-factors. These complexes modulate i.e. up-regulate or down-regulate the pattern of gene expres-sion. For example, if a gene is up-regulated, it is transcribed. This gene transcription leads to the biosynthesis of mRNA. The mRNA is detectable in the cell cytoplasm, and so the level of gene expression can be monitored using modern techniques of molecular genetics such as PCR (Polymerase Chain Reaction, which is a technique for copying and amplifying comple-mentary strands of a target DNA). Indeed, PCR is dependent on a RT (Reverse Transcriptase; an enzyme that makes a DNA copy of a segment of single-stranded RNA). Moreover, the mRNA leads to the biosynthesis of specific proteins; for example, those involved in bone formation (osteogenesis). The question now becomes: How do functional (Formational) appli-ances harness the physiologic mech-anism of signal transduction? The answer is a specific form of signal transduction called Mechanotrans-duction. In this case the signal that the cell receives is not a cytochemi-cal molecule but a mechanical or physical signal, such as stretch, deformation or a change in proprio-ceptive information. This change can be induced using the DNA appliance system or aligners etc. For example, when teeth meet in occlu-sion a certain amount of propriocep-tive information is exchanged, which keeps the teeth in a stable occlusal relationship. If an opposing tooth is extracted, the propriocep-tive information changes, and the change in spatial relations is detected by mechanoreceptors in the periodontium and periosteal membranes. This change in spatial relations produces signal transduc-tion, which ultimately leads to a change in the pattern of gene expression, mRNA biosynthesis etc., until a new position of stability is eventually reached (Fig. 1). This example succinctly encapsu-lates the central core of the Spatial Matrix Hypothesis. Moreover, changes in spatial relations induced when wearing functional (forma-tional) appliances stretch or compress soft and hard tissues of the craniofacial system. These changes are detected by mechanoreceptors in the periodontium and periosteal membranes, and the ensuing devel-opmental events can be harnessed for the correction of the malocclu-sion through the biosynthesis of new tissues, such as bone formation i.e. osteogenesis. Therefore, func-tional appliances might be better referred to as Formational appli-ances. But, how can this biologic phenomenon be controlled? Sutural Homeostasis During growth, the spatial and functional alignment of skeletal elements is maintained through remodeling of bony surfaces, including the periodontium, to permit function. For example, in a young child as the brain grows the calvaria are spread apart, and bone is deposited and remodeled to provide a protective covering for the expanding brain. But, environ-mentally-induced changes in the early morphologic relationship can produce a new solution or outcome. For example, native head-binding was practiced in certain South American cultures. The calvaria of these individuals appear deformed or abnormal compared to the normal skull morphology of that ethnicity, even though there was no functional deficit. Thus, departure from a genetically encoded ‘devel-opmental program’ leads to identifi-able abnormalities, which may or may not show dysfunction. For example, deformational (positional) plaigiocephaly is relatively common in some modern cultures. While the etiology of deforma-tional/positional plaigiocephaly is incompletely understood, changes in child-rearing practices may play a role. For example, laying the baby on a flat surface or in a child car-seat for prolonged periods may deform the calvaria, precipitating deformational/positional plaigio-cephaly. Applying this principle to structures caudal to the cranium, temporo-mandibular joint dysfunc-tion (TMD) may affect the jaw joints, malocclusions may affect the dentition, and obstructive sleep apnea (OSA) may affect the upper airway, etc. In each of these exam-ples, developmental compensation occurs to permit compromised func-tion, in accord with the Spatial Matrix Hypothesis. Therefore, a necessary first step in the treatment of TMD, malocclusions and OSA is decompensation. In other words, appropriate spatial signaling can re-establish (genomic) pattern forma-tion for optimal form and function. This change is spatial relations can be achieved by using functional (Formational) appliances such as the DNA appliance system prior to introducing aligners. Recent work on suture biology has elucidated the developmental mecha-nisms by which the above correc-tions might be achieved. First, it is important to understand that human sutures do not synostose even in adults 27 as previously thought. Second, a suture is a joint formed between two bones that undergo intramembranous ossification. In the embryo, sites of signal transduc-tion indicate locations where bone formation occurs de novo. These sites are often referred to as ‘ossification centers’. The ossification radiates outwards and eventually two skeletal elements come into close approxima-tion, for example as cranial sutures. It is now thought that sutures are subject to sutural homeostasis. Kambara 28 suggested that intermit-tent forces could: open a suture; stretch sutural connective tissues; induce new bone deposition, and be subject to homeostasis, which main-tained the sutural width. Put simply, www.orthodontics.com November/December 2010 23
Journal of the American Orthodontic Society November-December 2010: Page 23