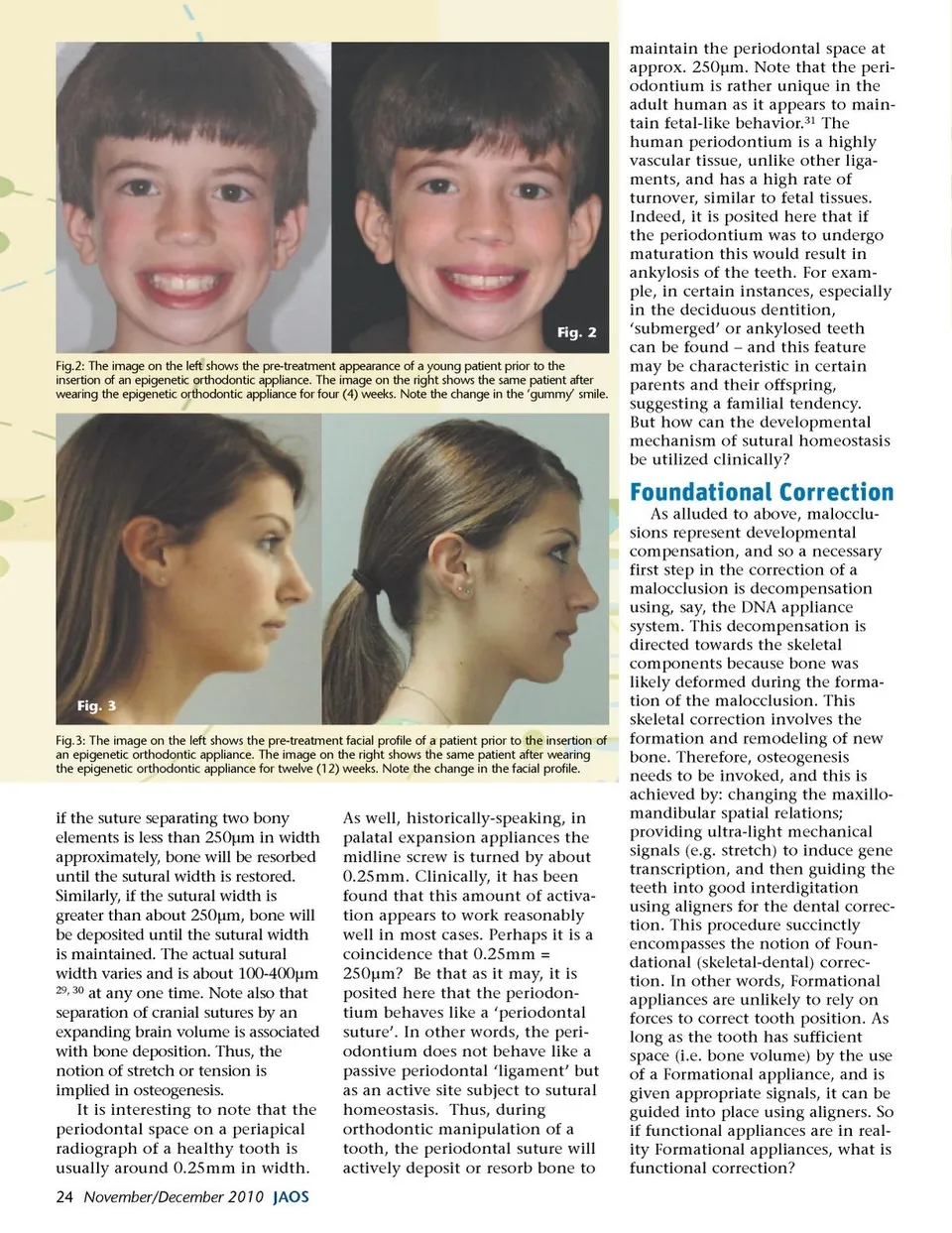
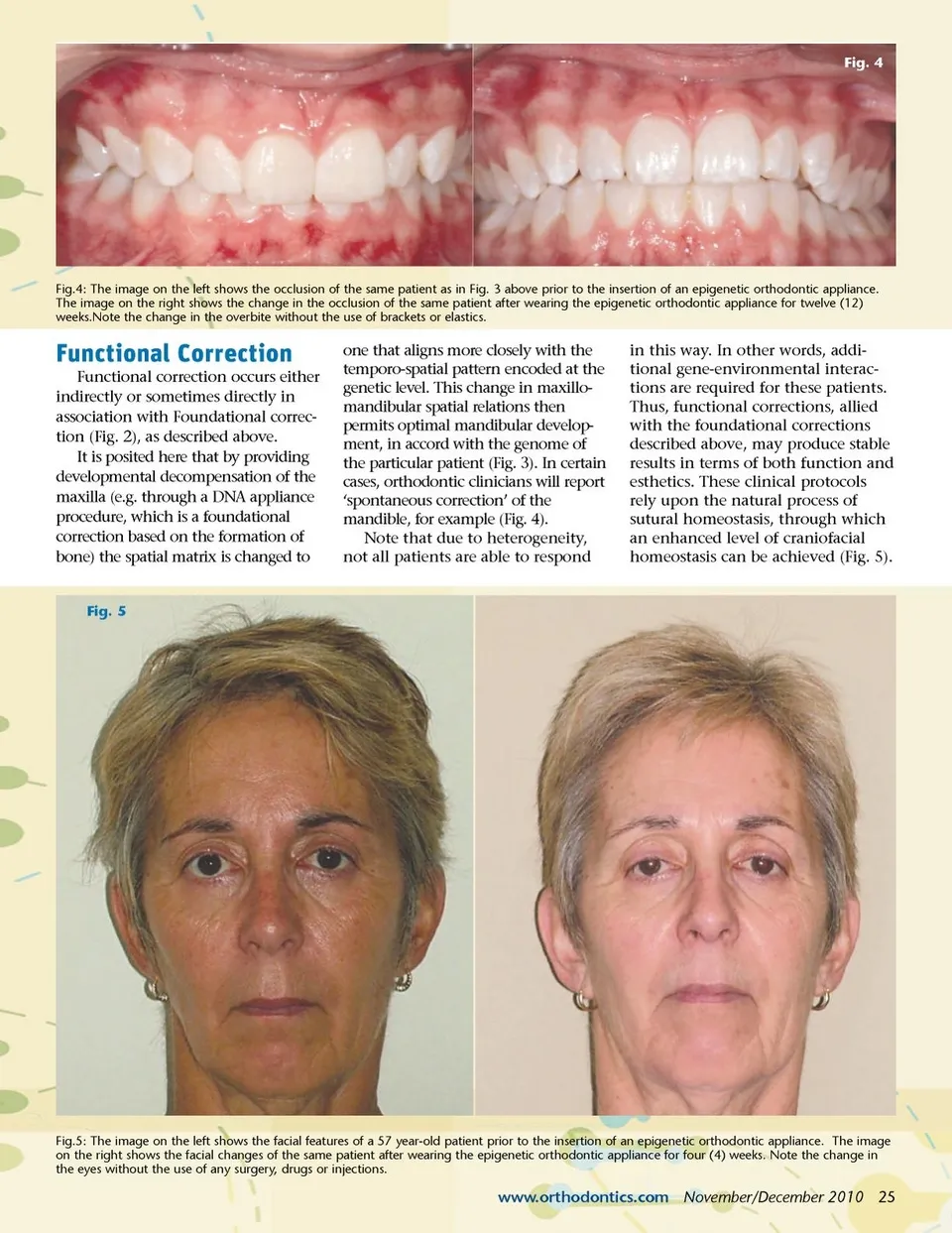
Fig. 2 Fig.2: The image on the left shows the pre-treatment appearance of a young patient prior to the insertion of an epigenetic orthodontic appliance. The image on the right shows the same patient after wearing the epigenetic orthodontic appliance for four (4) weeks. Note the change in the ‘gummy’ smile. maintain the periodontal space at approx. 250µm. Note that the peri-odontium is rather unique in the adult human as it appears to main-tain fetal-like behavior. 31 The human periodontium is a highly vascular tissue, unlike other liga-ments, and has a high rate of turnover, similar to fetal tissues. Indeed, it is posited here that if the periodontium was to undergo maturation this would result in ankylosis of the teeth. For exam-ple, in certain instances, especially in the deciduous dentition, ‘submerged’ or ankylosed teeth can be found – and this feature may be characteristic in certain parents and their offspring, suggesting a familial tendency. But how can the developmental mechanism of sutural homeostasis be utilized clinically? Foundational Correction As alluded to above, malocclu-sions represent developmental compensation, and so a necessary first step in the correction of a malocclusion is decompensation using, say, the DNA appliance system. This decompensation is directed towards the skeletal components because bone was likely deformed during the forma-tion of the malocclusion. This skeletal correction involves the formation and remodeling of new bone. Therefore, osteogenesis needs to be invoked, and this is achieved by: changing the maxillo-mandibular spatial relations; providing ultra-light mechanical signals (e.g. stretch) to induce gene transcription, and then guiding the teeth into good interdigitation using aligners for the dental correc-tion. This procedure succinctly encompasses the notion of Foun-dational (skeletal-dental) correc-tion. In other words, Formational appliances are unlikely to rely on forces to correct tooth position. As long as the tooth has sufficient space (i.e. bone volume) by the use of a Formational appliance, and is given appropriate signals, it can be guided into place using aligners. So if functional appliances are in real-ity Formational appliances, what is functional correction? Fig. 3 Fig.3: The image on the left shows the pre-treatment facial profile of a patient prior to the insertion of an epigenetic orthodontic appliance. The image on the right shows the same patient after wearing the epigenetic orthodontic appliance for twelve (12) weeks. Note the change in the facial profile. if the suture separating two bony elements is less than 250µm in width approximately, bone will be resorbed until the sutural width is restored. Similarly, if the sutural width is greater than about 250µm, bone will be deposited until the sutural width is maintained. The actual sutural width varies and is about 100-400µm 29, 30 at any one time. Note also that separation of cranial sutures by an expanding brain volume is associated with bone deposition. Thus, the notion of stretch or tension is implied in osteogenesis. It is interesting to note that the periodontal space on a periapical radiograph of a healthy tooth is usually around 0.25mm in width. 24 November/December 2010 JAOS As well, historically-speaking, in palatal expansion appliances the midline screw is turned by about 0.25mm. Clinically, it has been found that this amount of activa-tion appears to work reasonably well in most cases. Perhaps it is a coincidence that 0.25mm = 250µm? Be that as it may, it is posited here that the periodon-tium behaves like a ‘periodontal suture’. In other words, the peri-odontium does not behave like a passive periodontal ‘ligament’ but as an active site subject to sutural homeostasis. Thus, during orthodontic manipulation of a tooth, the periodontal suture will actively deposit or resorb bone to
Journal of the American Orthodontic Society November-December 2010: Page 24