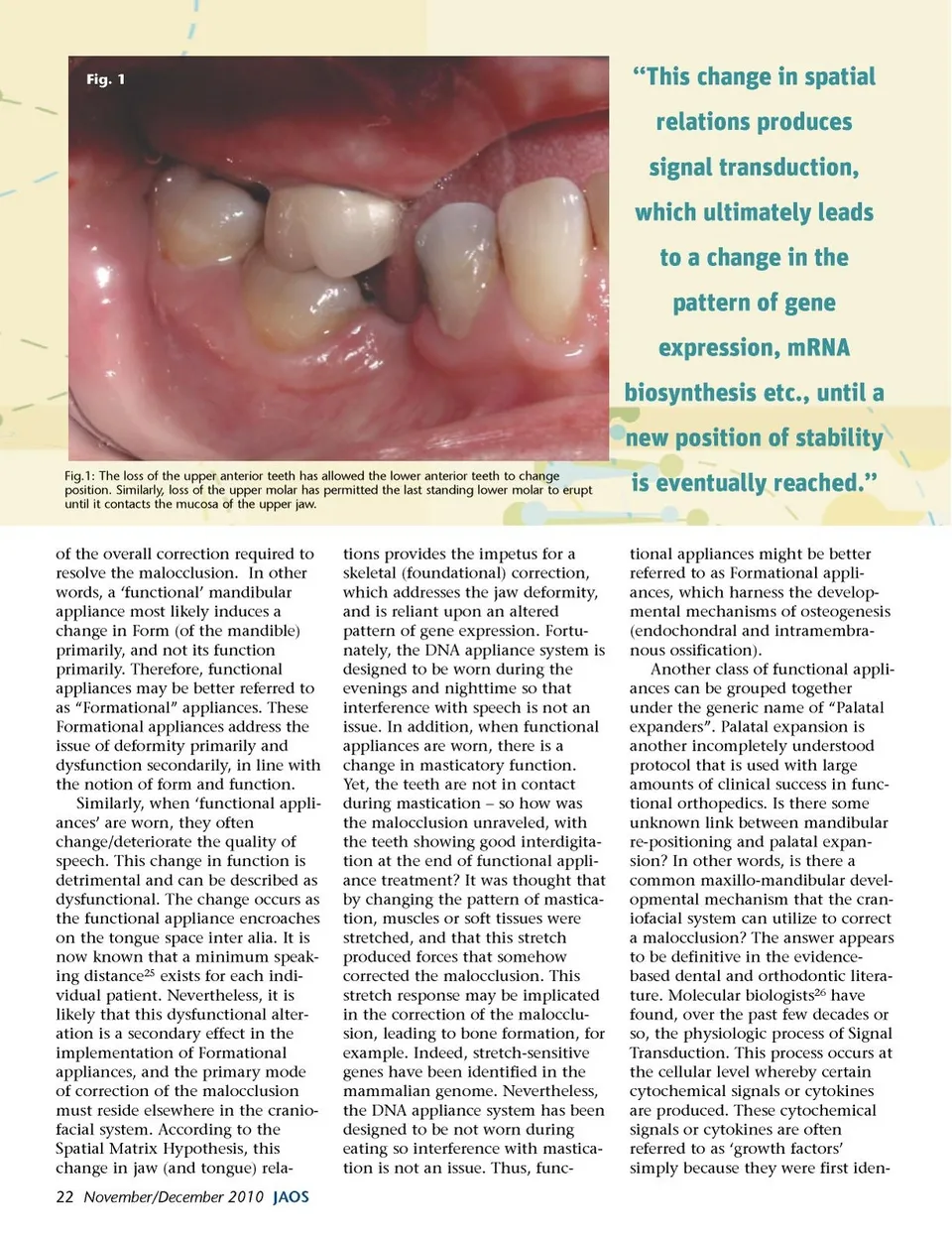
Fig. 1 “This change in spatial relations produces signal transduction, which ultimately leads to a change in the pattern of gene expression, mRNA biosynthesis etc., until a new position of stability Fig.1: The loss of the upper anterior teeth has allowed the lower anterior teeth to change position. Similarly, loss of the upper molar has permitted the last standing lower molar to erupt until it contacts the mucosa of the upper jaw. is eventually reached.” tional appliances might be better referred to as Formational appli-ances, which harness the develop-mental mechanisms of osteogenesis (endochondral and intramembra-nous ossification). Another class of functional appli-ances can be grouped together under the generic name of “Palatal expanders”. Palatal expansion is another incompletely understood protocol that is used with large amounts of clinical success in func-tional orthopedics. Is there some unknown link between mandibular re-positioning and palatal expan-sion? In other words, is there a common maxillo-mandibular devel-opmental mechanism that the cran-iofacial system can utilize to correct a malocclusion? The answer appears to be definitive in the evidence-based dental and orthodontic litera-ture. Molecular biologists 26 have found, over the past few decades or so, the physiologic process of Signal Transduction. This process occurs at the cellular level whereby certain cytochemical signals or cytokines are produced. These cytochemical signals or cytokines are often referred to as ‘growth factors’ simply because they were first iden-of the overall correction required to resolve the malocclusion. In other words, a ‘functional’ mandibular appliance most likely induces a change in Form (of the mandible) primarily, and not its function primarily. Therefore, functional appliances may be better referred to as “Formational” appliances. These Formational appliances address the issue of deformity primarily and dysfunction secondarily, in line with the notion of form and function. Similarly, when ‘functional appli-ances’ are worn, they often change/deteriorate the quality of speech. This change in function is detrimental and can be described as dysfunctional. The change occurs as the functional appliance encroaches on the tongue space inter alia. It is now known that a minimum speak-ing distance 25 exists for each indi-vidual patient. Nevertheless, it is likely that this dysfunctional alter-ation is a secondary effect in the implementation of Formational appliances, and the primary mode of correction of the malocclusion must reside elsewhere in the cranio-facial system. According to the Spatial Matrix Hypothesis, this change in jaw (and tongue) rela-22 November/December 2010 JAOS tions provides the impetus for a skeletal (foundational) correction, which addresses the jaw deformity, and is reliant upon an altered pattern of gene expression. Fortu-nately, the DNA appliance system is designed to be worn during the evenings and nighttime so that interference with speech is not an issue. In addition, when functional appliances are worn, there is a change in masticatory function. Yet, the teeth are not in contact during mastication – so how was the malocclusion unraveled, with the teeth showing good interdigita-tion at the end of functional appli-ance treatment? It was thought that by changing the pattern of mastica-tion, muscles or soft tissues were stretched, and that this stretch produced forces that somehow corrected the malocclusion. This stretch response may be implicated in the correction of the malocclu-sion, leading to bone formation, for example. Indeed, stretch-sensitive genes have been identified in the mammalian genome. Nevertheless, the DNA appliance system has been designed to be not worn during eating so interference with mastica-tion is not an issue. Thus, func-
Journal of the American Orthodontic Society November-December 2010: Page 22