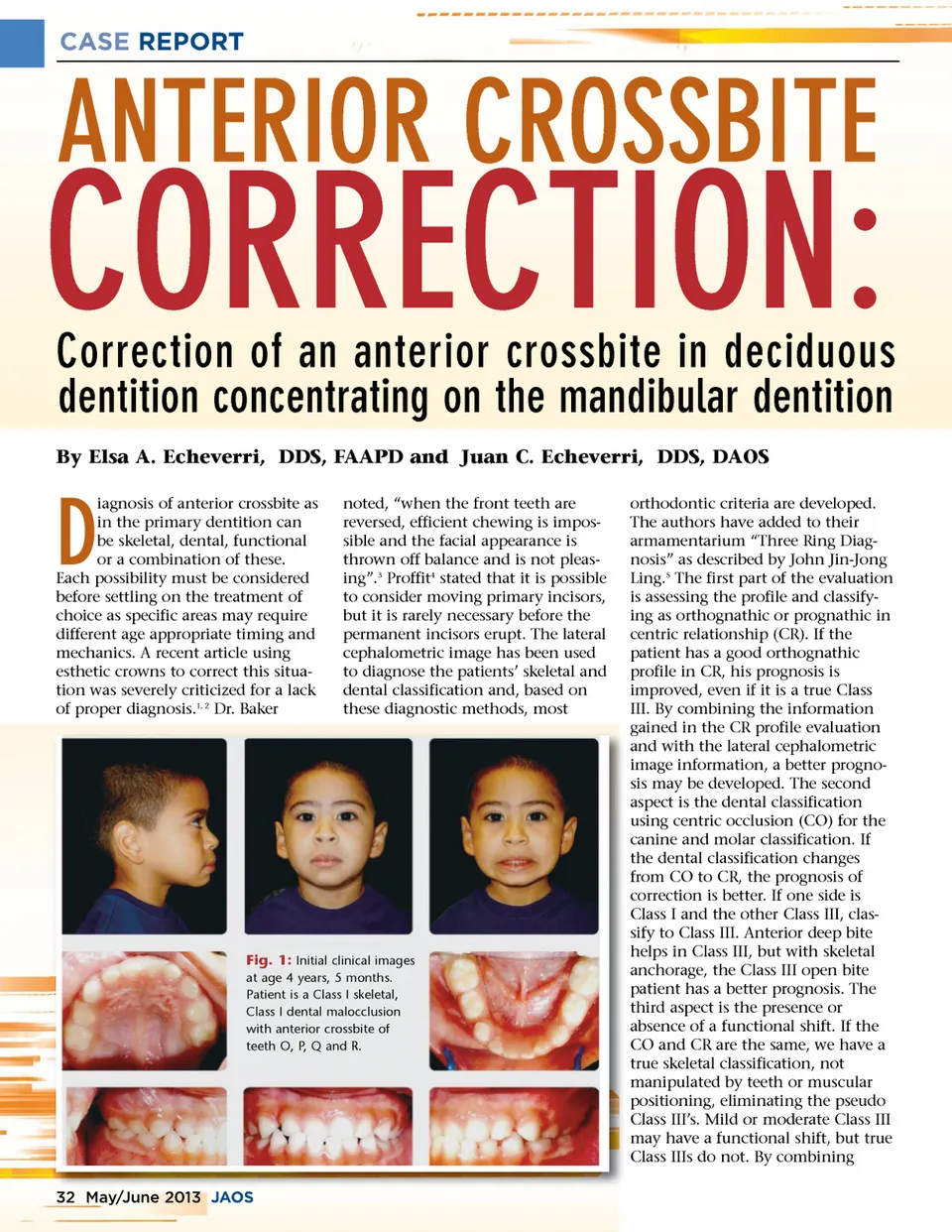
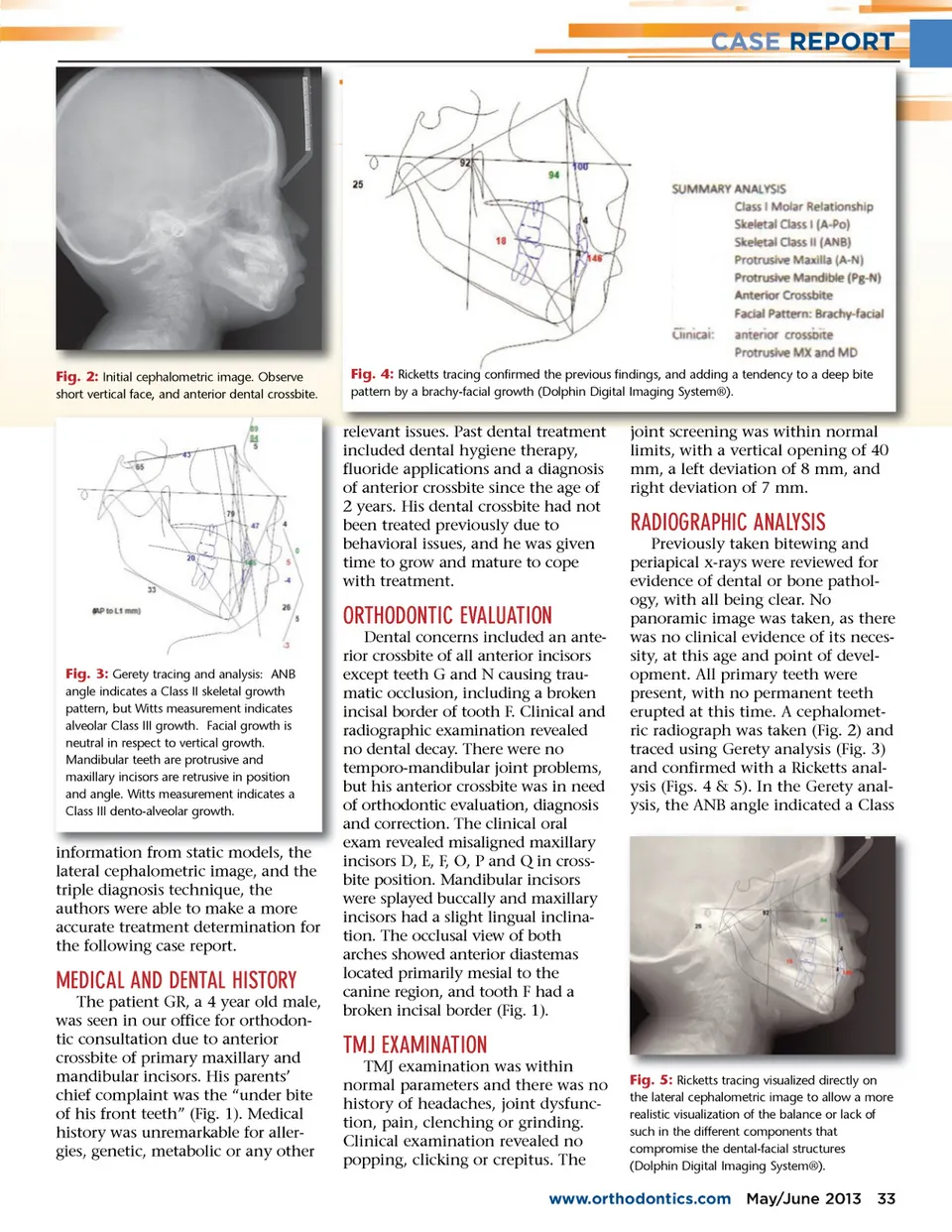
CASE REPORT Fig. 2: Initial cephalometric image. Observe short vertical face, and anterior dental crossbite. Fig. 4: Ricketts tracing confirmed the previous findings, and adding a tendency to a deep bite pattern by a brachy-facial growth (Dolphin Digital Imaging System®). relevant rel levant t issues. i ssues Past P ast t dental d ent tal l treatment t reat tment t included dental hygiene therapy, fluoride applications and a diagnosis of anterior crossbite since the age of 2 years. His dental crossbite had not been treated previously due to behavioral issues, and he was given time to grow and mature to cope with treatment. j oi int t screening screeni ing was within wi it h i n normal l joint limits, with a vertical opening of 40 mm, a left deviation of 8 mm, and right deviation of 7 mm. RADIOGRAPHIC ANALYSIS Previously taken bitewing and periapical x-rays were reviewed for evidence of dental or bone pathol-ogy, with all being clear. No panoramic image was taken, as there was no clinical evidence of its neces-sity, at this age and point of devel-opment. All primary teeth were present, with no permanent teeth erupted at this time. A cephalomet-ric radiograph was taken (Fig. 2) and traced using Gerety analysis (Fig. 3) and confirmed with a Ricketts anal-ysis (Figs. 4 & 5). In the Gerety anal-ysis, the ANB angle indicated a Class ORTHODONTIC EVALUATION Fig. 3: Gerety tracing and analysis: ANB angle indicates a Class II skeletal growth pattern, but Witts measurement indicates alveolar Class III growth. Facial growth is neutral in respect to vertical growth. Mandibular teeth are protrusive and maxillary incisors are retrusive in position and angle. Witts measurement indicates a Class III dento-alveolar growth. from models, the information fr f om static models lateral cephalometric image, and the triple diagnosis technique, the authors were able to make a more accurate treatment determination for the following case report. MEDICAL AND DENTAL HISTORY The patient GR, a 4 year old male, was seen in our office for orthodon-tic consultation due to anterior crossbite of primary maxillary and mandibular incisors. His parents’ chief complaint was the “under bite of his front teeth” (Fig. 1). Medical history was unremarkable for aller-gies, genetic, metabolic or any other Dental concerns included an ante-rior crossbite of all anterior incisors except teeth G and N causing trau-matic occlusion, including a broken incisal border of tooth F. Clinical and radiographic examination revealed no dental decay. There were no temporo-mandibular joint problems, but his anterior crossbite was in need of orthodontic evaluation, diagnosis and correction. The clinical oral exam revealed misaligned maxillary incisors D, E, F, O, P and Q in cross-bite position. Mandibular incisors were splayed buccally and maxillary incisors had a slight lingual inclina-tion. The occlusal view of both arches showed anterior diastemas located primarily mesial to the canine region, and tooth F had a broken incisal border (Fig. 1). TMJ EXAMINATION TMJ examination was within normal parameters and there was no history of headaches, joint dysfunc-tion, pain, clenching or grinding. Clinical examination revealed no popping, clicking or crepitus. The Fig. 5: Ricketts tracing visualized directly on the lateral cephalometric image to allow a more realistic visualization of the balance or lack of such in the different components that compromise the dental-facial structures (Dolphin Digital Imaging System®). www.orthodontics.com May/June 2013 33
Journal of the American Orthodontic Society May-June 2013: Page 33