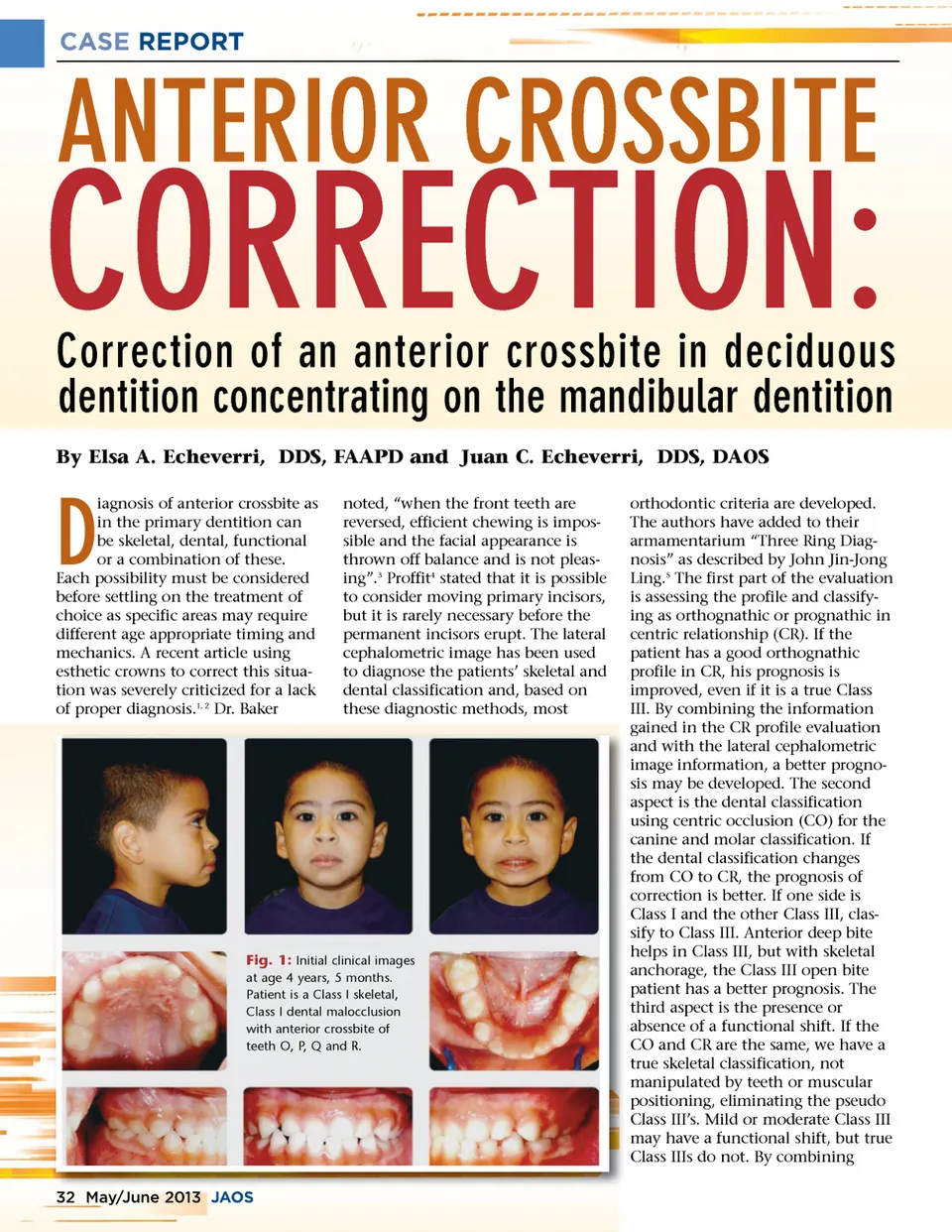
CASE REPORT CORRECTION: By Elsa A. Echeverri, DDS, FAAPD and Juan C. Echeverri, DDS, DAOS ANTERIOR CROSSBITE Correction of an anterior crossbite in deciduous dentition concentrating on the mandibular dentition noted, “when the front teeth are reversed, efficient chewing is impos-sible and the facial appearance is thrown off balance and is not pleas-ing”. 3 Proffit 4 stated that it is possible to consider moving primary incisors, but it is rarely necessary before the permanent incisors erupt. The lateral cephalometric image has been used to diagnose the patients’ skeletal and dental classification and, based on these diagnostic methods, most orthodontic criteria are developed. The authors have added to their armamentarium “Three Ring Diag-nosis” as described by John Jin-Jong Ling. 5 The first part of the evaluation is assessing the profile and classify-ing as orthognathic or prognathic in centric relationship (CR). If the patient has a good orthognathic profile in CR, his prognosis is improved, even if it is a true Class III. By combining the information gained in the CR profile evaluation and with the lateral cephalometric image information, a better progno-sis may be developed. The second aspect is the dental classification using centric occlusion (CO) for the canine and molar classification. If the dental classification changes from CO to CR, the prognosis of correction is better. If one side is Class I and the other Class III, clas-sify to Class III. Anterior deep bite helps in Class III, but with skeletal anchorage, the Class III open bite patient has a better prognosis. The third aspect is the presence or absence of a functional shift. If the CO and CR are the same, we have a true skeletal classification, not manipulated by teeth or muscular positioning, eliminating the pseudo Class III’s. Mild or moderate Class III may have a functional shift, but true Class IIIs do not. By combining D iagnosis of anterior crossbite as in the primary dentition can be skeletal, dental, functional or a combination of these. Each possibility must be considered before settling on the treatment of choice as specific areas may require different age appropriate timing and mechanics. A recent article using esthetic crowns to correct this situa-tion was severely criticized for a lack of proper diagnosis. 1, 2 Dr. Baker Fig. 1: Initial clinical images at age 4 years, 5 months. Patient is a Class I skeletal, Class I dental malocclusion with anterior crossbite of teeth O, P, Q and R. 32 May/June / 2013 0 JAOS O
Journal of the American Orthodontic Society May-June 2013: Page 32