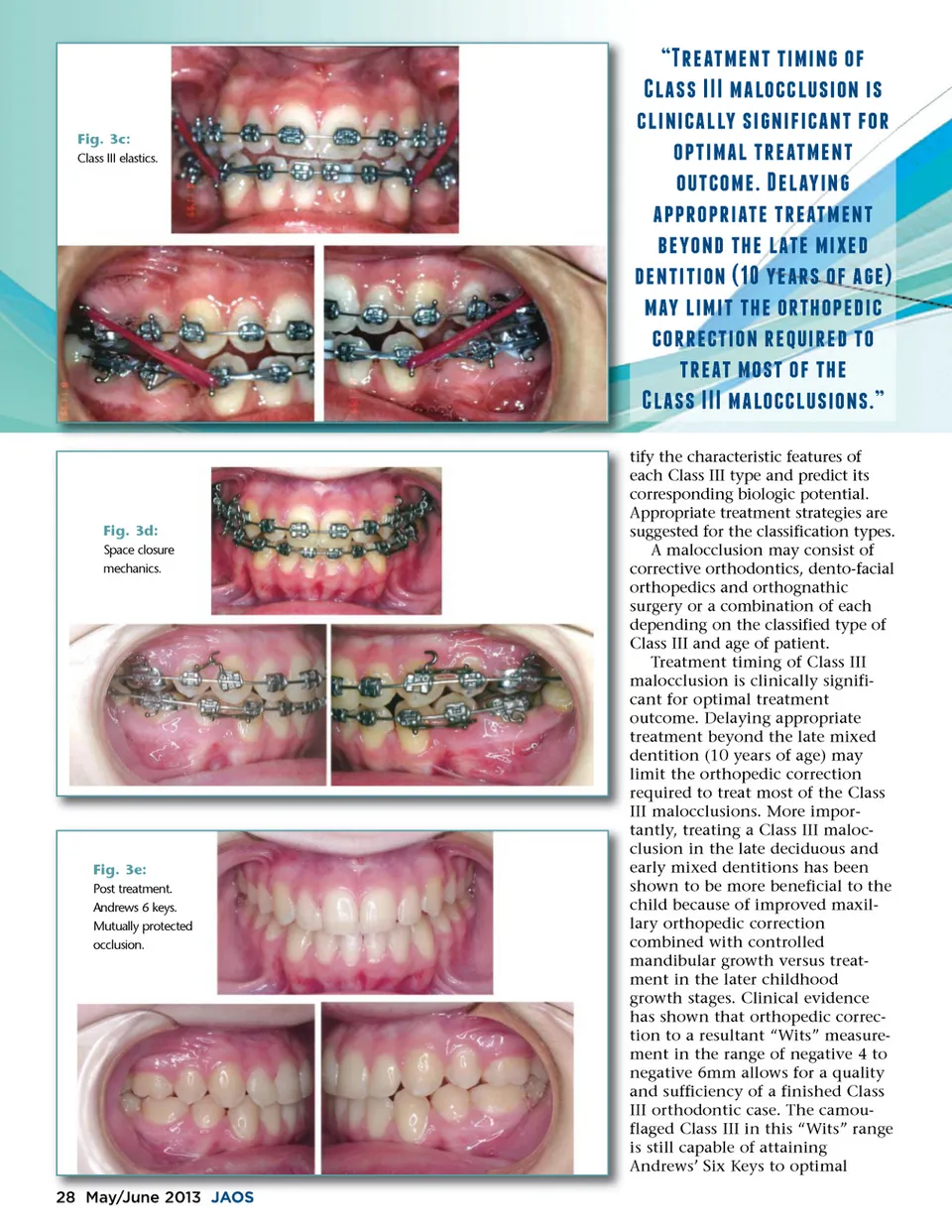
Fig. 3c: Class III elastics. a;*/.1&/+1210&0+ 2-% c;).,,2###2&.)-(()!,0-+20, ()0+0(.))f;2,0 +0%0(.+12%-* -"10&.)21*/.1&/+1 -!1(-&/2 /).f;0+ .""*-"*0.1/21*/.1&/+1 e;/f;-+'21$/2).1/2&0/' '/+1010-+2�e;2f;/.*,2-%2. / &.f;2)0&0121$/2-*1$-"/'0( (-**/(10-+2*/ !0*/'21-1*/.12&-,12-%21$/ c;).,,2###2&.)-(()!,0-+,�f; tify the characteristic features of each Class III type and predict its corresponding biologic potential. Appropriate treatment strategies are suggested for the classification types. A malocclusion may consist of corrective orthodontics, dento-facial orthopedics and orthognathic surgery or a combination of each depending on the classified type of Class III and age of patient. Treatment timing of Class III malocclusion is clinically signifi-cant for optimal treatment outcome. Delaying appropriate treatment beyond the late mixed dentition (10 years of age) may limit the orthopedic correction required to treat most of the Class III malocclusions. More impor-tantly, treating a Class III maloc-clusion in the late deciduous and early mixed dentitions has been shown to be more beneficial to the child because of improved maxil-lary orthopedic correction combined with controlled mandibular growth versus treat-ment in the later childhood growth stages. Clinical evidence has shown that orthopedic correc-tion to a resultant “Wits” measure-ment in the range of negative 4 to negative 6mm allows for a quality and sufficiency of a finished Class III orthodontic case. The camou-flaged Class III in this “Wits” range is still capable of attaining Andrews’ Six Keys to optimal Fig. 3d: Space closure mechanics. Fig. 3e: Post treatment. Andrews 6 keys. Mutually protected occlusion. 28 May/June May/ y / J une 2013 JA JAOS OS
Journal of the American Orthodontic Society May-June 2013: Page 28