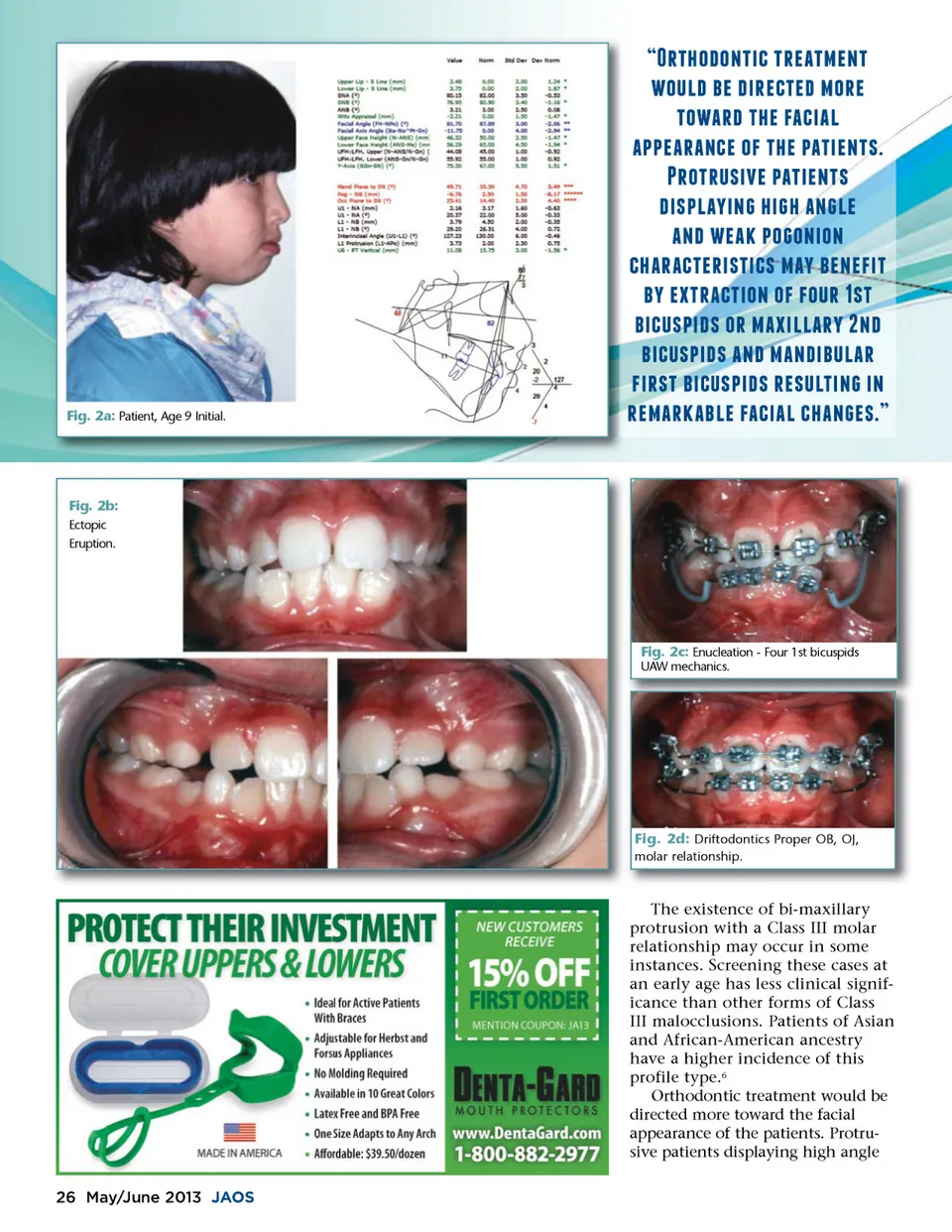
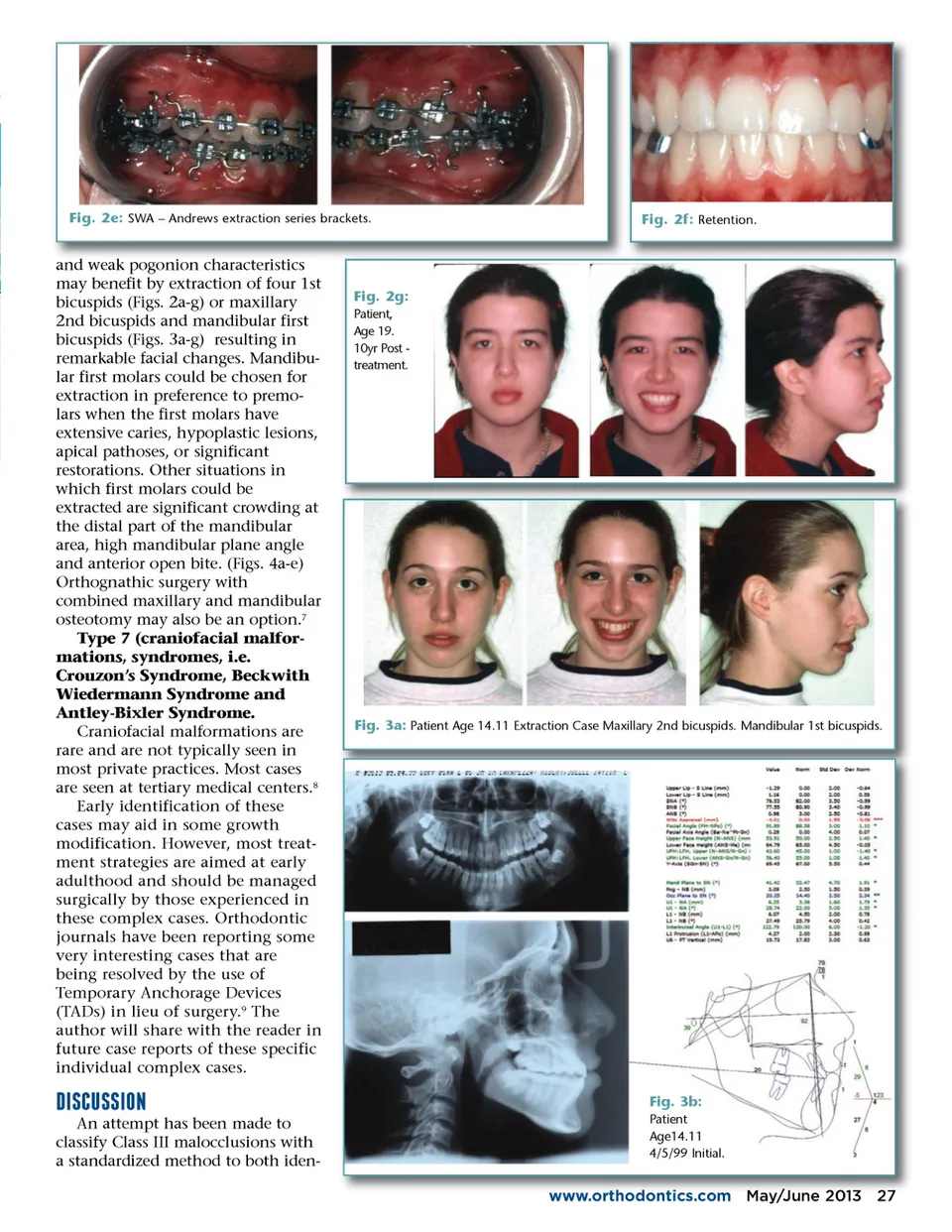
Fig. 2a: Patient, Age 9 Initial. *1$-'-+10(21*/.1&/+1 -!)'2e;/2'0*/(1/'2&-*/ 1-.*'21$/2%.(0.) .""/.*.+(/2-%21$/2".10/+1, *-1*!,0�a;/2".10/+1, '0,").f;0+ 2$0 $2.+ )/ .+'2/.�b;2"--+0-+ ($.*.(1/*0,10(,2&.f;2e;/+/%01 e;f;2/1*.(10-+2-%2%-!*2�e;,1 e;0(!,"0',2-*2&.0)).*f;2+' e;0(!,"0',2.+'2&.+'0e;!).* %0*,12e;0(!,"0',2*/,!)10+ 20+ */&.*�b;.e;)/2%.(0.)2($.+ /,�f; Fig. 2b: Ectopic Eruption. Fig. 2c: Enucleation -Four 1st bicuspids UAW mechanics. Fig. 2d: Driftodontics Proper OB, OJ, molar relationship. The existence of bi-maxillary protrusion with a Class III molar relationship may occur in some instances. Screening these cases at an early age has less clinical signif-icance than other forms of Class III malocclusions. Patients of Asian and African-American ancestry have a higher incidence of this profile type. 6 Orthodontic treatment would be directed more toward the facial appearance of the patients. Protru-sive patients displaying high angle 26 May/June 2013 JAOS
Journal of the American Orthodontic Society May-June 2013: Page 26