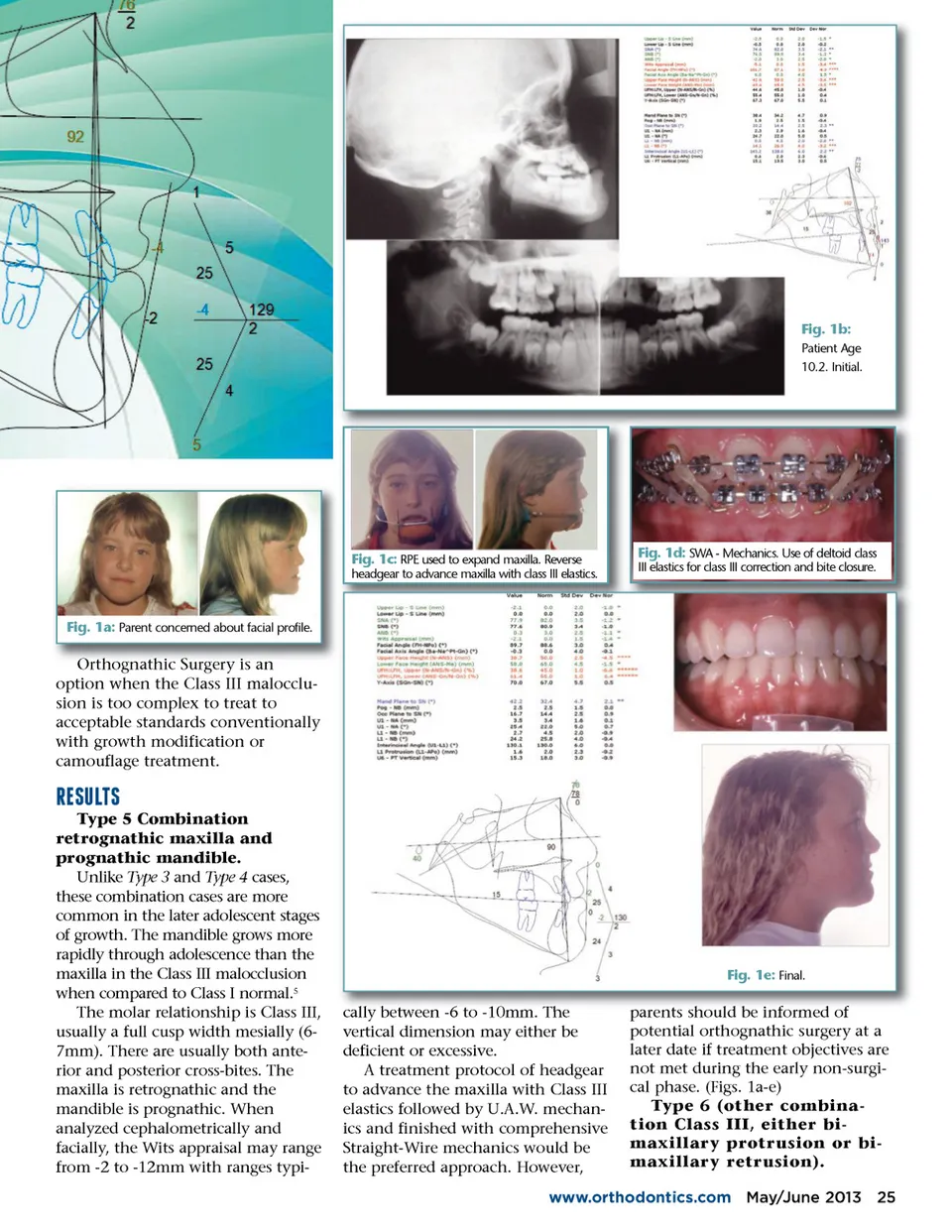
Fig. 1b: Patient Age 10.2. Initial. Fig. 1c: RPE used to expand maxilla. Reverse headgear to advance maxilla with class III elastics. Fig. 1d: SWA -Mechanics. Use of deltoid class III elastics for class III correction and bite closure. Fig. 1a: Parent concerned about facial profile. Orthognathic Surgery is an option when the Class III malocclu-sion is too complex to treat to acceptable standards conventionally with growth modification or camouflage treatment. b;d;a;d;22 Type 5 Combination retrognathic maxilla and prognathic mandible. Unlike Type 3 and Type 4 cases, these combination cases are more common in the later adolescent stages of growth. The mandible grows more rapidly through adolescence than the maxilla in the Class III malocclusion when compared to Class I normal. 5 The molar relationship is Class III, usually a full cusp width mesially (6-7mm). There are usually both ante-rior and posterior cross-bites. The maxilla is retrognathic and the mandible is prognathic. When analyzed cephalometrically and facially, the Wits appraisal may range from -2 to -12mm with ranges typi-Fig. 1e: Final. cally between -6 6 to -10mm. 10mm The vertical dimension may either be deficient or excessive. A treatment protocol of headgear to advance the maxilla with Class III elastics followed by U.A.W. mechan-ics and finished with comprehensive Straight-Wire mechanics would be the preferred approach. However, parents should be informed of potential orthognathic surgery at a later date if treatment objectives are not met during the early non-surgi-cal phase. (Figs. 1a-e) Type 6 (other combina-tion Class III, either bi-maxillary protrusion or bi-maxillary retrusion). www.orthodontics.com May/June 2013 25
Journal of the American Orthodontic Society May-June 2013: Page 25