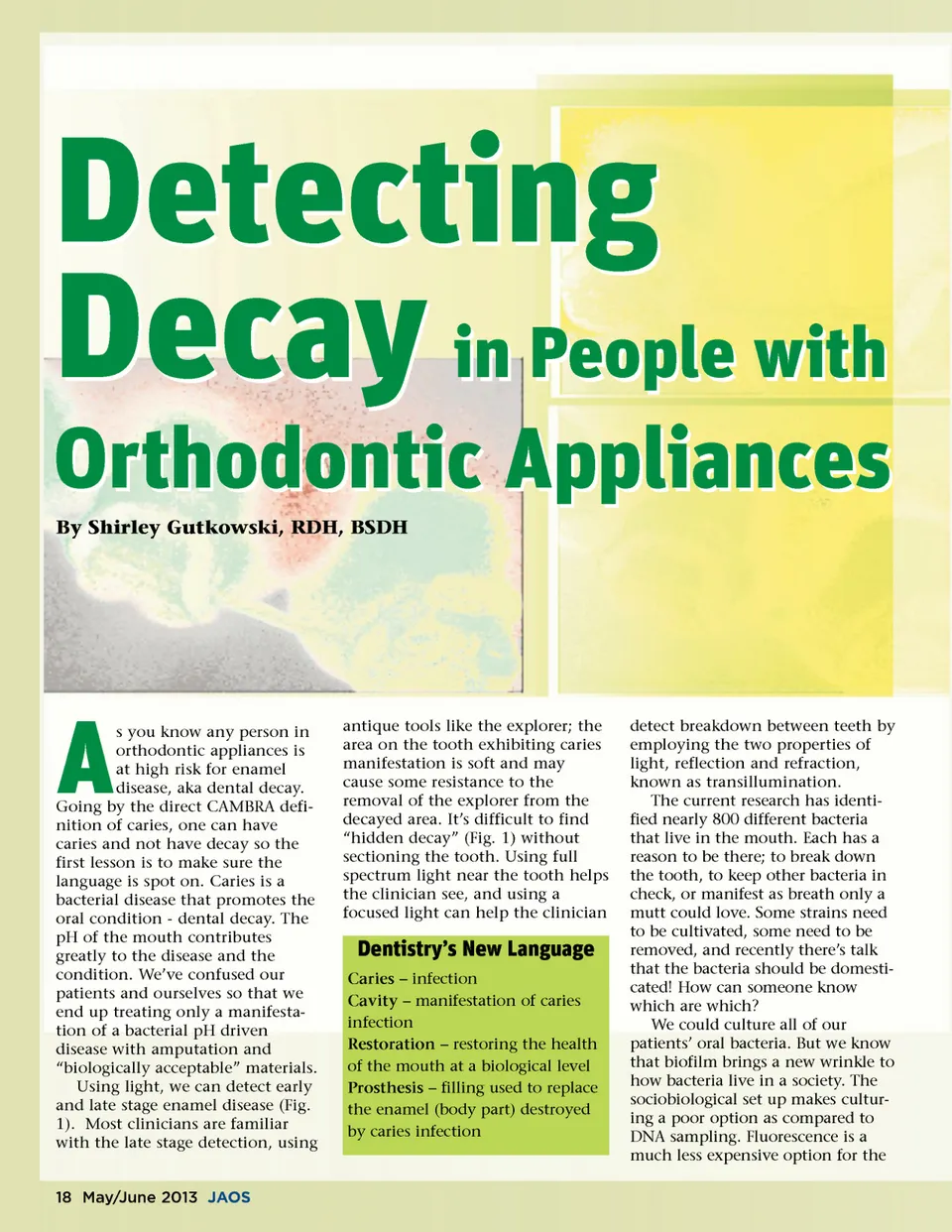
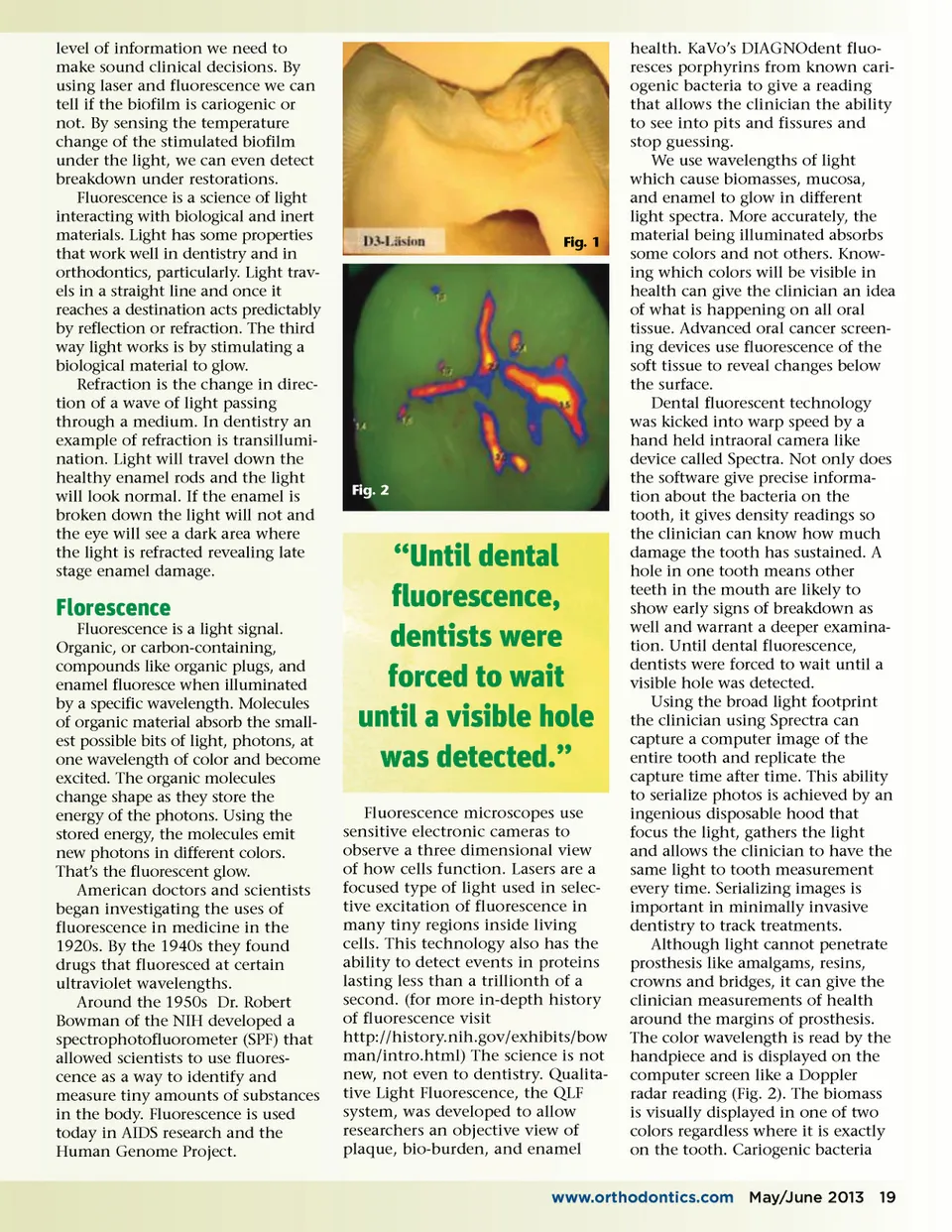
level of information we need to make sound clinical decisions. By using laser and fluorescence we can tell if the biofilm is cariogenic or not. By sensing the temperature change of the stimulated biofilm under the light, we can even detect breakdown under restorations. Fluorescence is a science of light interacting with biological and inert materials. Light has some properties that work well in dentistry and in orthodontics, particularly. Light trav-els in a straight line and once it reaches a destination acts predictably by reflection or refraction. The third way light works is by stimulating a biological material to glow. Refraction is the change in direc-tion of a wave of light passing through a medium. In dentistry an example of refraction is transillumi-nation. Light will travel down the healthy enamel rods and the light will look normal. If the enamel is broken down the light will not and the eye will see a dark area where the light is refracted revealing late stage enamel damage. Fig. 1 Fig. 2 Florescence Fluorescence is a light signal. Organic, or carbon-containing, compounds like organic plugs, and enamel fluoresce when illuminated by a specific wavelength. Molecules of organic material absorb the small-est possible bits of light, photons, at one wavelength of color and become excited. The organic molecules change shape as they store the energy of the photons. Using the stored energy, the molecules emit new photons in different colors. That’s the fluorescent glow. American doctors and scientists began investigating the uses of fluorescence in medicine in the 1920s. By the 1940s they found drugs that fluoresced at certain ultraviolet wavelengths. Around the 1950s Dr. Robert Bowman of the NIH developed a spectrophotofluorometer (SPF) that allowed scientists to use fluores-cence as a way to identify and measure tiny amounts of substances in the body. Fluorescence is used today in AIDS research and the Human Genome Project. “Until dental fluorescence, dentists were forced to wait until a visible hole was detected.” Fluorescence microscopes use sensitive electronic cameras to observe a three dimensional view of how cells function. Lasers are a focused type of light used in selec-tive excitation of fluorescence in many tiny regions inside living cells. This technology also has the ability to detect events in proteins lasting less than a trillionth of a second. (for more in-depth history of fluorescence visit http://history.nih.gov/exhibits/bow man/intro.html) The science is not new, not even to dentistry. Qualita-tive Light Fluorescence, the QLF system, was developed to allow researchers an objective view of plaque, bio-burden, and enamel health. KaVo’s DIAGNOdent fluo-resces porphyrins from known cari-ogenic bacteria to give a reading that allows the clinician the ability to see into pits and fissures and stop guessing. We use wavelengths of light which cause biomasses, mucosa, and enamel to glow in different light spectra. More accurately, the material being illuminated absorbs some colors and not others. Know-ing which colors will be visible in health can give the clinician an idea of what is happening on all oral tissue. Advanced oral cancer screen-ing devices use fluorescence of the soft tissue to reveal changes below the surface. Dental fluorescent technology was kicked into warp speed by a hand held intraoral camera like device called Spectra. Not only does the software give precise informa-tion about the bacteria on the tooth, it gives density readings so the clinician can know how much damage the tooth has sustained. A hole in one tooth means other teeth in the mouth are likely to show early signs of breakdown as well and warrant a deeper examina-tion. Until dental fluorescence, dentists were forced to wait until a visible hole was detected. Using the broad light footprint the clinician using Sprectra can capture a computer image of the entire tooth and replicate the capture time after time. This ability to serialize photos is achieved by an ingenious disposable hood that focus the light, gathers the light and allows the clinician to have the same light to tooth measurement every time. Serializing images is important in minimally invasive dentistry to track treatments. Although light cannot penetrate prosthesis like amalgams, resins, crowns and bridges, it can give the clinician measurements of health around the margins of prosthesis. The color wavelength is read by the handpiece and is displayed on the computer screen like a Doppler radar reading (Fig. 2). The biomass is visually displayed in one of two colors regardless where it is exactly on the tooth. Cariogenic bacteria www.orthodontics.com May/June 2013 19
Journal of the American Orthodontic Society May-June 2013: Page 19