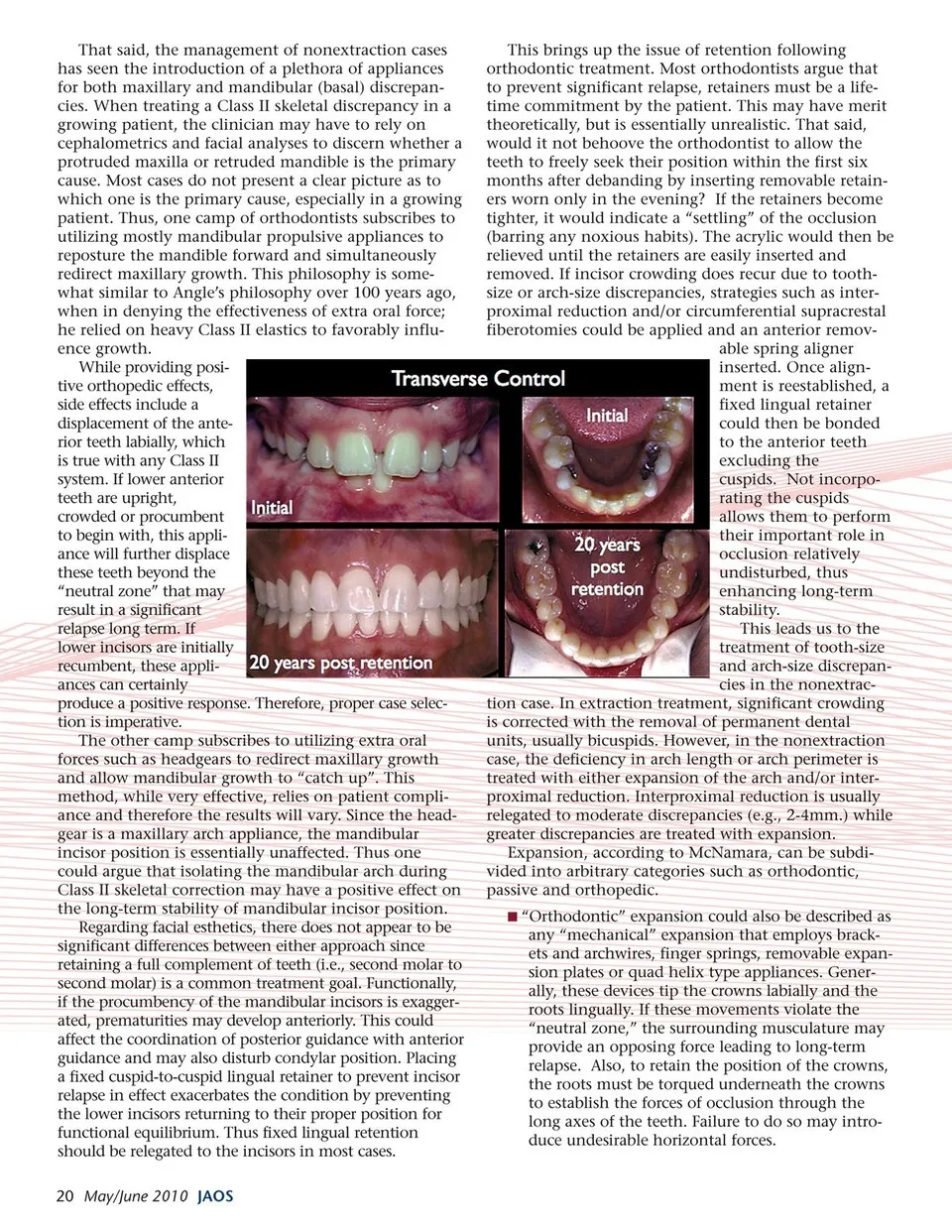
That said, the management of nonextraction cases has seen the introduction of a plethora of appliances for both maxillary and mandibular (basal) discrepan- cies. When treating a Class II skeletal discrepancy in a growing patient, the clinician may have to rely on cephalometrics and facial analyses to discern whether a protruded maxilla or retruded mandible is the primary cause. Most cases do not present a clear picture as to which one is the primary cause, especially in a growing patient. Thus, one camp of orthodontists subscribes to utilizing mostly mandibular propulsive appliances to reposture the mandible forward and simultaneously redirect maxillary growth. This philosophy is some- what similar to Angle’s philosophy over 100 years ago, when in denying the effectiveness of extra oral force; he relied on heavy Class II elastics to favorably influ- ence growth. While providing posi- tive orthopedic effects, side effects include a displacement of the ante- rior teeth labially, which is true with any Class II system. If lower anterior teeth are upright, crowded or procumbent to begin with, this appli- ance will further displace these teeth beyond the “neutral zone” that may result in a significant relapse long term. If lower incisors are initially recumbent, these appli- ances can certainly produce a positive response. Therefore, proper case selec- tion is imperative. The other camp subscribes to utilizing extra oral forces such as headgears to redirect maxillary growth and allow mandibular growth to “catch up”. This method, while very effective, relies on patient compli- ance and therefore the results will vary. Since the head- gear is a maxillary arch appliance, the mandibular incisor position is essentially unaffected. Thus one could argue that isolating the mandibular arch during Class II skeletal correction may have a positive effect on the long-term stability of mandibular incisor position. Regarding facial esthetics, there does not appear to be significant differences between either approach since retaining a full complement of teeth (i.e., second molar to second molar) is a common treatment goal. Functionally, if the procumbency of the mandibular incisors is exagger- ated, prematurities may develop anteriorly. This could affect the coordination of posterior guidance with anterior guidance and may also disturb condylar position. Placing a fixed cuspid-to-cuspid lingual retainer to prevent incisor relapse in effect exacerbates the condition by preventing the lower incisors returning to their proper position for functional equilibrium. Thus fixed lingual retention should be relegated to the incisors in most cases. 20 May/June 2010 JAOS This brings up the issue of retention following orthodontic treatment. Most orthodontists argue that to prevent significant relapse, retainers must be a life- time commitment by the patient. This may have merit theoretically, but is essentially unrealistic. That said, would it not behoove the orthodontist to allow the teeth to freely seek their position within the first six months after debanding by inserting removable retain- ers worn only in the evening? If the retainers become tighter, it would indicate a “settling” of the occlusion (barring any noxious habits). The acrylic would then be relieved until the retainers are easily inserted and removed. If incisor crowding does recur due to tooth- size or arch-size discrepancies, strategies such as inter- proximal reduction and/or circumferential supracrestal fiberotomies could be applied and an anterior remov- able spring aligner inserted. Once align- ment is reestablished, a fixed lingual retainer could then be bonded to the anterior teeth excluding the cuspids. Not incorpo- rating the cuspids allows them to perform their important role in occlusion relatively undisturbed, thus enhancing long-term stability. This leads us to the treatment of tooth-size and arch-size discrepan- cies in the nonextrac- tion case. In extraction treatment, significant crowding is corrected with the removal of permanent dental units, usually bicuspids. However, in the nonextraction case, the deficiency in arch length or arch perimeter is treated with either expansion of the arch and/or inter- proximal reduction. Interproximal reduction is usually relegated to moderate discrepancies (e.g., 2-4mm.) while greater discrepancies are treated with expansion. Expansion, according to McNamara, can be subdi- vided into arbitrary categories such as orthodontic, passive and orthopedic. “Orthodontic” expansion could also be described as any “mechanical” expansion that employs brack- ets and archwires, finger springs, removable expan- sion plates or quad helix type appliances. Gener- ally, these devices tip the crowns labially and the roots lingually. If these movements violate the “neutral zone,” the surrounding musculature may provide an opposing force leading to long-term relapse. Also, to retain the position of the crowns, the roots must be torqued underneath the crowns to establish the forces of occlusion through the long axes of the teeth. Failure to do so may intro- duce undesirable horizontal forces.
Journal of the American Orthodontic Society May-June 2010: Page 20