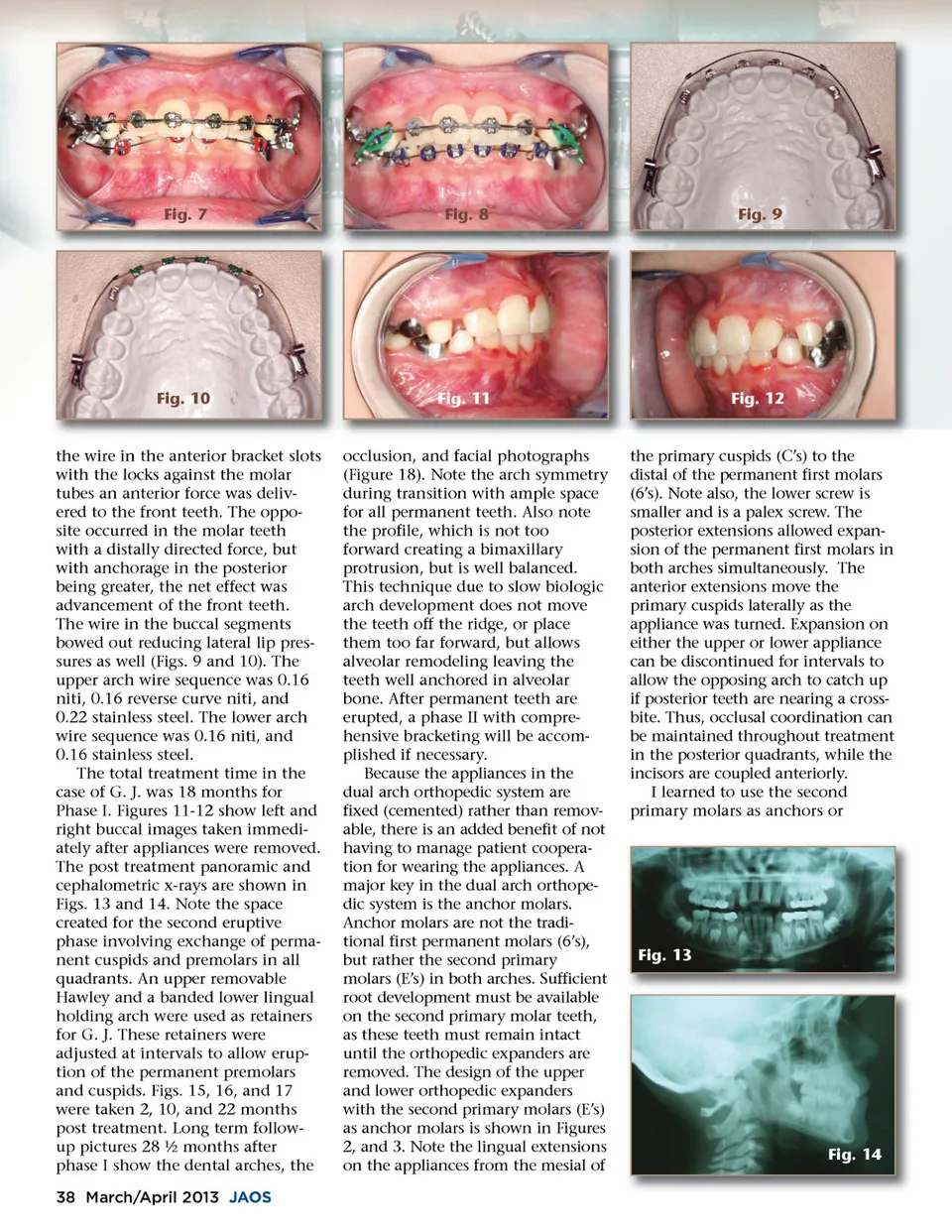
Fig. 7 Fig. 8 Fig. 9 Fig. 10 Fig. 11 Fig. 12 the wire in the anterior bracket slots with the locks against the molar tubes an anterior force was deliv-ered to the front teeth. The oppo-site occurred in the molar teeth with a distally directed force, but with anchorage in the posterior being greater, the net effect was advancement of the front teeth. The wire in the buccal segments bowed out reducing lateral lip pres-sures as well (Figs. 9 and 10). The upper arch wire sequence was 0.16 niti, 0.16 reverse curve niti, and 0.22 stainless steel. The lower arch wire sequence was 0.16 niti, and 0.16 stainless steel. The total treatment time in the case of G. J. was 18 months for Phase I. Figures 11-12 show left and right buccal images taken immedi-ately after appliances were removed. The post treatment panoramic and cephalometric x-rays are shown in Figs. 13 and 14. Note the space created for the second eruptive phase involving exchange of perma-nent cuspids and premolars in all quadrants. An upper removable Hawley and a banded lower lingual holding arch were used as retainers for G. J. These retainers were adjusted at intervals to allow erup-tion of the permanent premolars and cuspids. Figs. 15, 16, and 17 were taken 2, 10, and 22 months post treatment. Long term follow-up pictures 28 ½ months after phase I show the dental arches, the 38 March/April 2013 JAOS occlusion, and facial photographs (Figure 18). Note the arch symmetry during transition with ample space for all permanent teeth. Also note the profile, which is not too forward creating a bimaxillary protrusion, but is well balanced. This technique due to slow biologic arch development does not move the teeth off the ridge, or place them too far forward, but allows alveolar remodeling leaving the teeth well anchored in alveolar bone. After permanent teeth are erupted, a phase II with compre-hensive bracketing will be accom-plished if necessary. Because the appliances in the dual arch orthopedic system are fixed (cemented) rather than remov-able, there is an added benefit of not having to manage patient coopera-tion for wearing the appliances. A major key in the dual arch orthope-dic system is the anchor molars. Anchor molars are not the tradi-tional first permanent molars (6’s), but rather the second primary molars (E’s) in both arches. Sufficient root development must be available on the second primary molar teeth, as these teeth must remain intact until the orthopedic expanders are removed. The design of the upper and lower orthopedic expanders with the second primary molars (E’s) as anchor molars is shown in Figures 2, and 3. Note the lingual extensions on the appliances from the mesial of the primary cuspids (C’s) to the distal of the permanent first molars (6’s). Note also, the lower screw is smaller and is a palex screw. The posterior extensions allowed expan-sion of the permanent first molars in both arches simultaneously. The anterior extensions move the primary cuspids laterally as the appliance was turned. Expansion on either the upper or lower appliance can be discontinued for intervals to allow the opposing arch to catch up if posterior teeth are nearing a cross-bite. Thus, occlusal coordination can be maintained throughout treatment in the posterior quadrants, while the incisors are coupled anteriorly. I learned to use the second primary molars as anchors or Fig. 13 Fig. 14
Journal of the American Orthodontic Society March-April 2013: Page 38