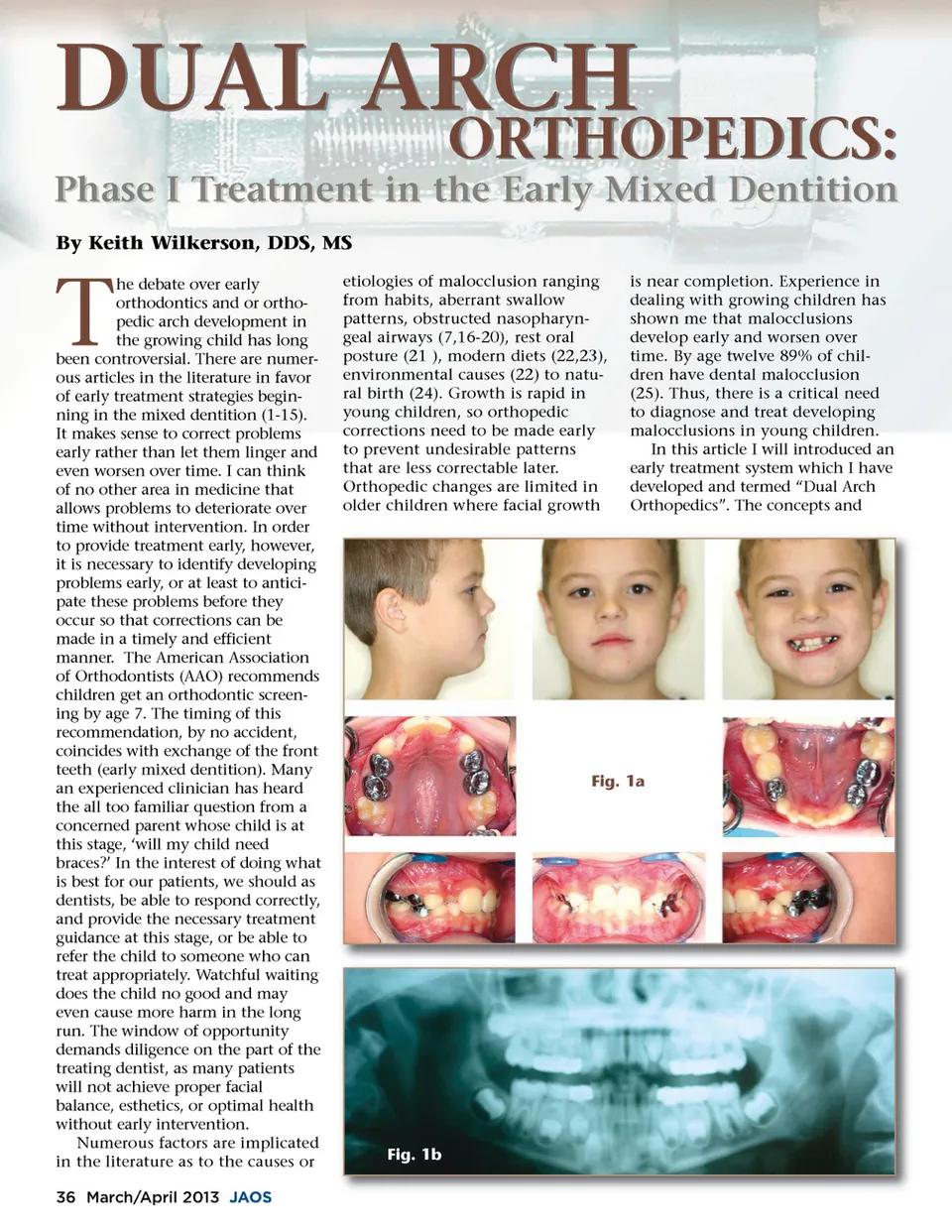
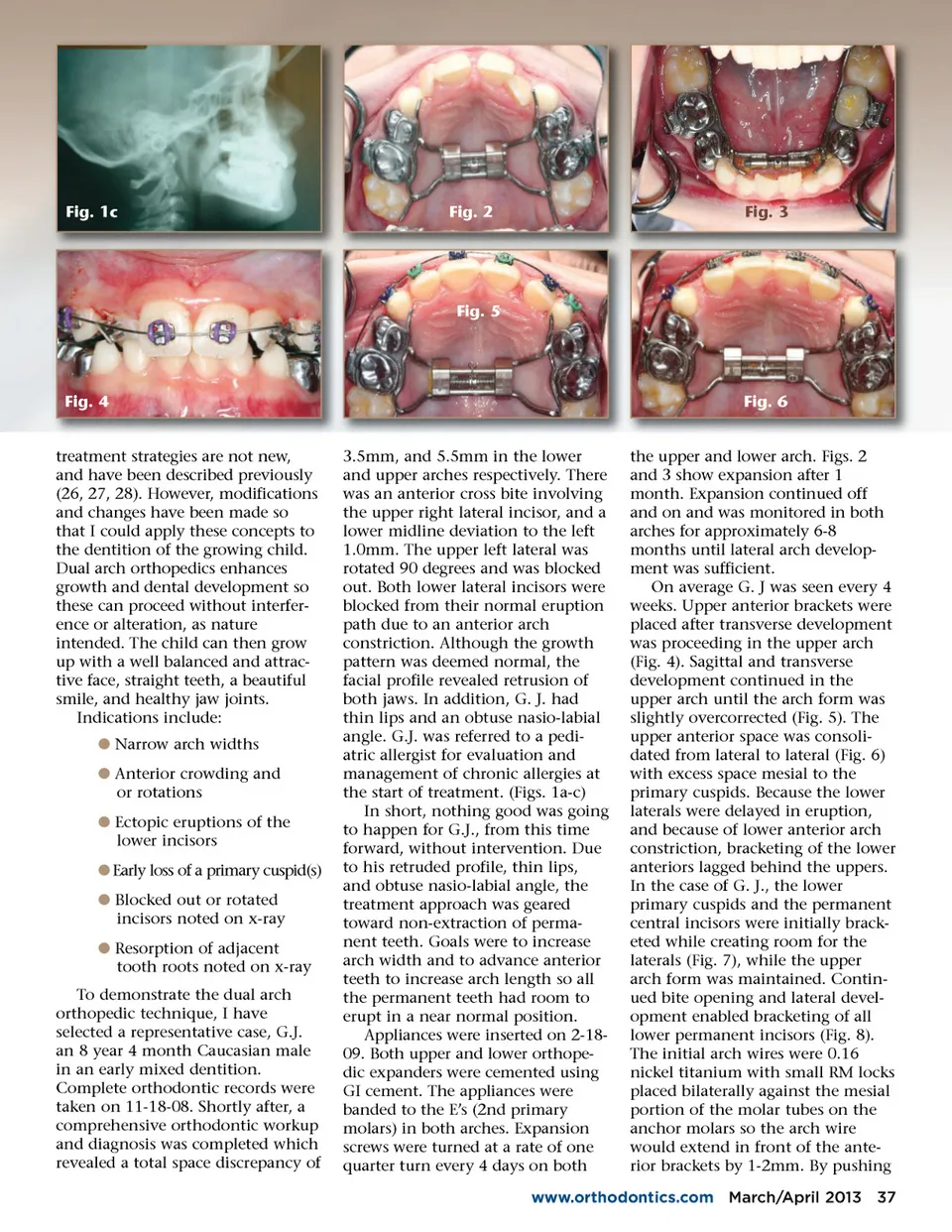
Fig. 1c Fig. 2 Fig. 3 Fig. 5 Fig. 4 Fig. 6 treatment strategies are not new, and have been described previously (26, 27, 28). However, modifications and changes have been made so that I could apply these concepts to the dentition of the growing child. Dual arch orthopedics enhances growth and dental development so these can proceed without interfer-ence or alteration, as nature intended. The child can then grow up with a well balanced and attrac-tive face, straight teeth, a beautiful smile, and healthy jaw joints. Indications include: b Narrow arch widths b Anterior crowding and or rotations b Ectopic eruptions of the lower incisors b Early loss of a primary cuspid(s) b Blocked out or rotated incisors noted on x-ray b Resorption of adjacent tooth roots noted on x-ray To demonstrate the dual arch orthopedic technique, I have selected a representative case, G.J. an 8 year 4 month Caucasian male in an early mixed dentition. Complete orthodontic records were taken on 11-18-08. Shortly after, a comprehensive orthodontic workup and diagnosis was completed which revealed a total space discrepancy of 3.5mm, and 5.5mm in the lower and upper arches respectively. There was an anterior cross bite involving the upper right lateral incisor, and a lower midline deviation to the left 1.0mm. The upper left lateral was rotated 90 degrees and was blocked out. Both lower lateral incisors were blocked from their normal eruption path due to an anterior arch constriction. Although the growth pattern was deemed normal, the facial profile revealed retrusion of both jaws. In addition, G. J. had thin lips and an obtuse nasio-labial angle. G.J. was referred to a pedi-atric allergist for evaluation and management of chronic allergies at the start of treatment. (Figs. 1a-c) In short, nothing good was going to happen for G.J., from this time forward, without intervention. Due to his retruded profile, thin lips, and obtuse nasio-labial angle, the treatment approach was geared toward non-extraction of perma-nent teeth. Goals were to increase arch width and to advance anterior teeth to increase arch length so all the permanent teeth had room to erupt in a near normal position. Appliances were inserted on 2-18-09. Both upper and lower orthope-dic expanders were cemented using GI cement. The appliances were banded to the E’s (2nd primary molars) in both arches. Expansion screws were turned at a rate of one quarter turn every 4 days on both the upper and lower arch. Figs. 2 and 3 show expansion after 1 month. Expansion continued off and on and was monitored in both arches for approximately 6-8 months until lateral arch develop-ment was sufficient. On average G. J was seen every 4 weeks. Upper anterior brackets were placed after transverse development was proceeding in the upper arch (Fig. 4). Sagittal and transverse development continued in the upper arch until the arch form was slightly overcorrected (Fig. 5). The upper anterior space was consoli-dated from lateral to lateral (Fig. 6) with excess space mesial to the primary cuspids. Because the lower laterals were delayed in eruption, and because of lower anterior arch constriction, bracketing of the lower anteriors lagged behind the uppers. In the case of G. J., the lower primary cuspids and the permanent central incisors were initially brack-eted while creating room for the laterals (Fig. 7), while the upper arch form was maintained. Contin-ued bite opening and lateral devel-opment enabled bracketing of all lower permanent incisors (Fig. 8). The initial arch wires were 0.16 nickel titanium with small RM locks placed bilaterally against the mesial portion of the molar tubes on the anchor molars so the arch wire would extend in front of the ante-rior brackets by 1-2mm. By pushing www.orthodontics.com March/April 2013 37
Journal of the American Orthodontic Society March-April 2013: Page 37