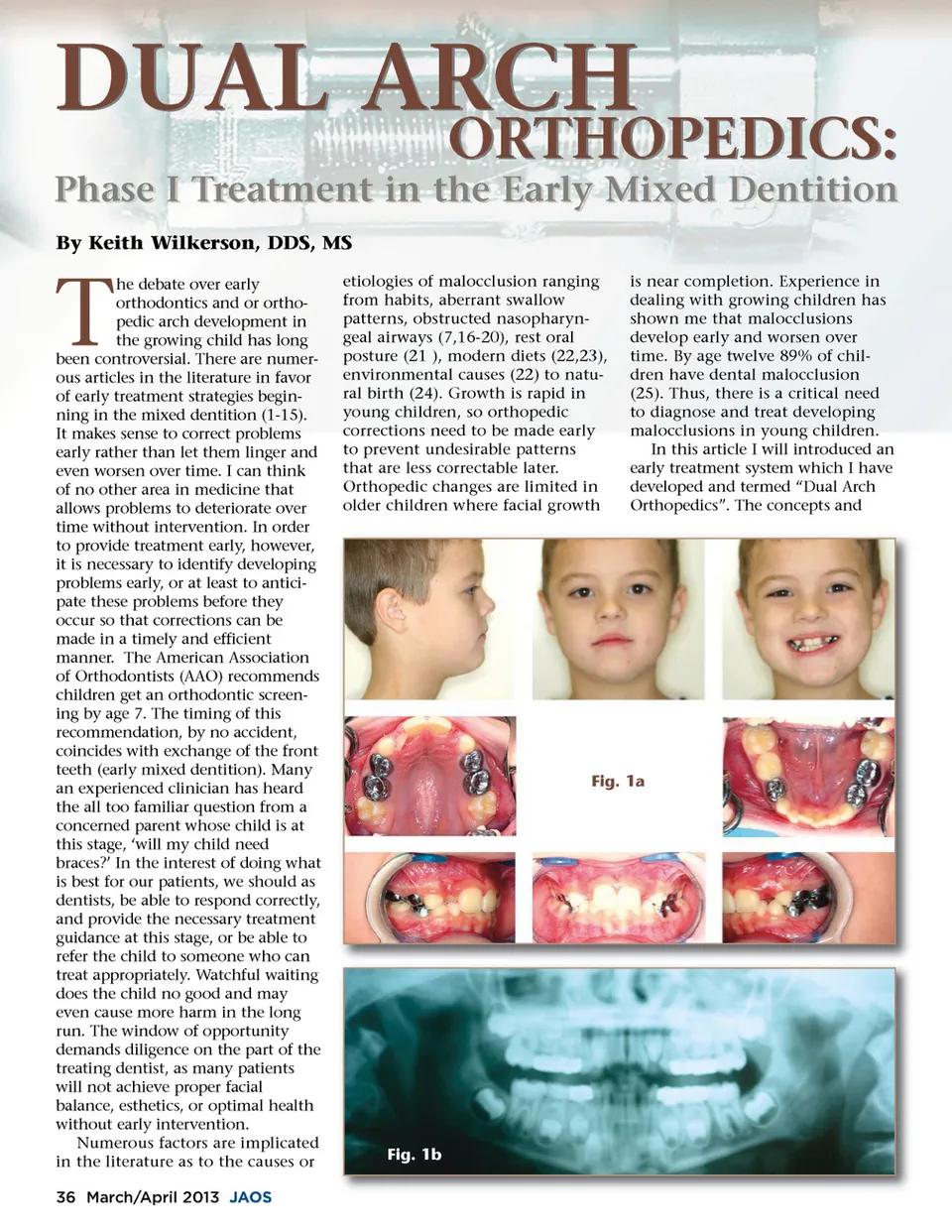
DUAL ARCH By Keith Wilkerson, DDS, MS ORTHOPEDICS: is near completion. Experience in dealing with growing children has shown me that malocclusions develop early and worsen over time. By age twelve 89% of chil-dren have dental malocclusion (25). Thus, there is a critical need to diagnose and treat developing malocclusions in young children. In this article I will introduced an early treatment system which I have developed and termed “Dual Arch Orthopedics”. The concepts and Phase I Treatment in the Early Mixed Dentition T he debate over early orthodontics and or ortho-pedic arch development in the growing child has long been controversial. There are numer-ous articles in the literature in favor of early treatment strategies begin-ning in the mixed dentition (1-15). It makes sense to correct problems early rather than let them linger and even worsen over time. I can think of no other area in medicine that allows problems to deteriorate over time without intervention. In order to provide treatment early, however, it is necessary to identify developing problems early, or at least to antici-pate these problems before they occur so that corrections can be made in a timely and efficient manner. The American Association of Orthodontists (AAO) recommends children get an orthodontic screen-ing by age 7. The timing of this recommendation, by no accident, coincides with exchange of the front teeth (early mixed dentition). Many an experienced clinician has heard the all too familiar question from a concerned parent whose child is at this stage, ‘will my child need braces?’ In the interest of doing what is best for our patients, we should as dentists, be able to respond correctly, and provide the necessary treatment guidance at this stage, or be able to refer the child to someone who can treat appropriately. Watchful waiting does the child no good and may even cause more harm in the long run. The window of opportunity demands diligence on the part of the treating dentist, as many patients will not achieve proper facial balance, esthetics, or optimal health without early intervention. Numerous factors are implicated in the literature as to the causes or 36 March/April 2013 JAOS etiologies of malocclusion ranging from habits, aberrant swallow patterns, obstructed nasopharyn-geal airways (7,16-20), rest oral posture (21 ), modern diets (22,23), environmental causes (22) to natu-ral birth (24). Growth is rapid in young children, so orthopedic corrections need to be made early to prevent undesirable patterns that are less correctable later. Orthopedic changes are limited in older children where facial growth Fig. 1a Fig. 1b
Journal of the American Orthodontic Society March-April 2013: Page 36