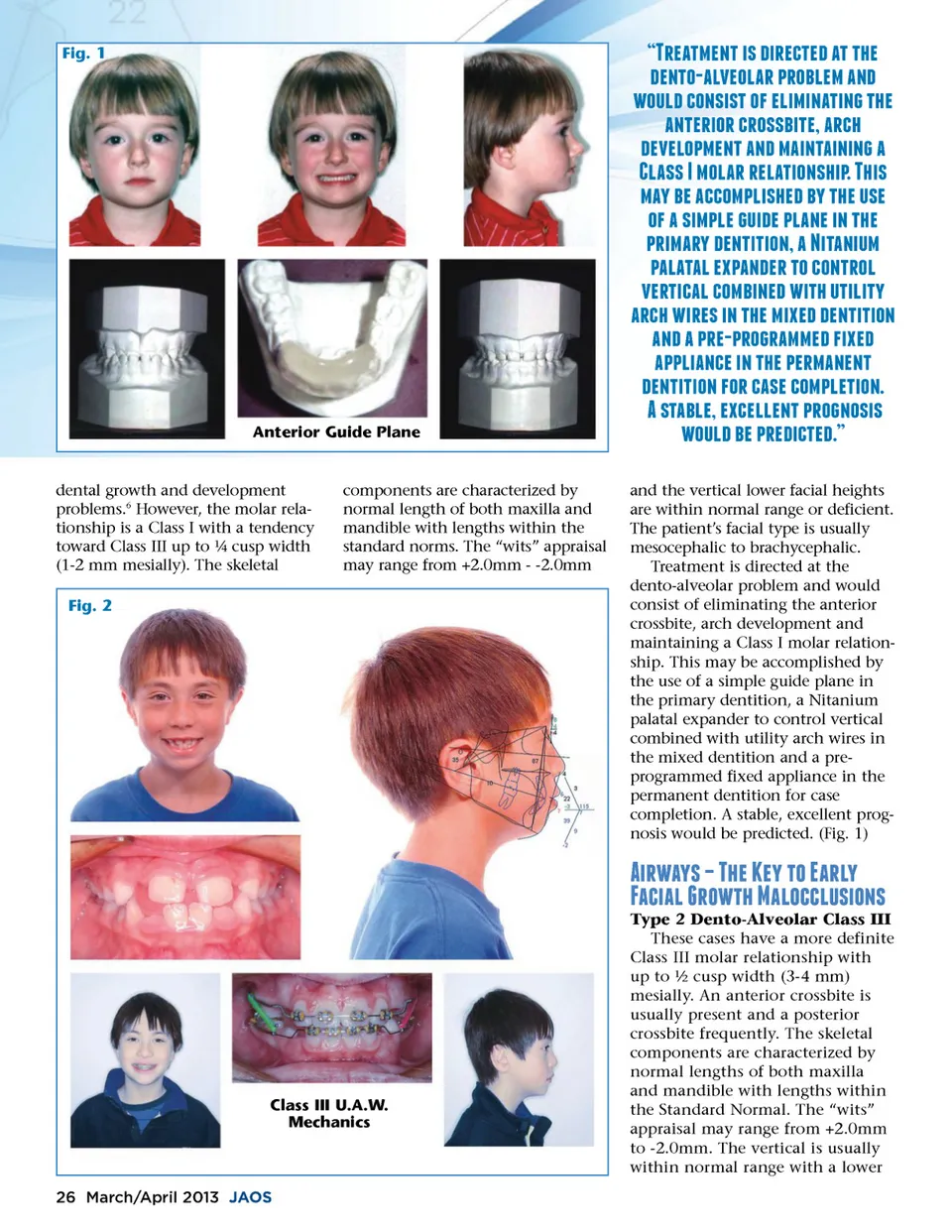
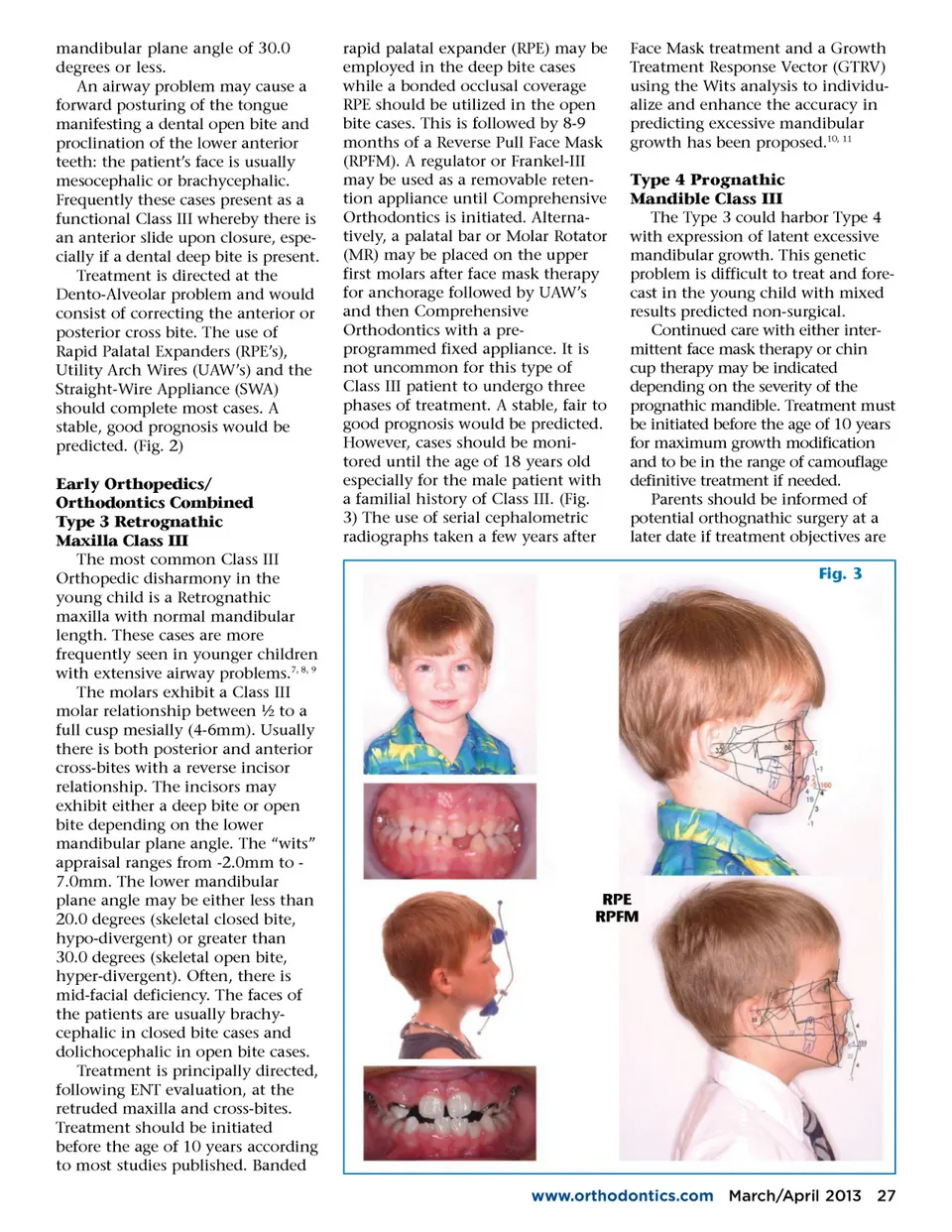
mandibular plane angle of 30.0 degrees or less. An airway problem may cause a forward posturing of the tongue manifesting a dental open bite and proclination of the lower anterior teeth: the patient’s face is usually mesocephalic or brachycephalic. Frequently these cases present as a functional Class III whereby there is an anterior slide upon closure, espe-cially if a dental deep bite is present. Treatment is directed at the Dento-Alveolar problem and would consist of correcting the anterior or posterior cross bite. The use of Rapid Palatal Expanders (RPE’s), Utility Arch Wires (UAW’s) and the Straight-Wire Appliance (SWA) should complete most cases. A stable, good prognosis would be predicted. (Fig. 2) Early Orthopedics/ Orthodontics Combined Type 3 Retrognathic Maxilla Class III The most common Class III Orthopedic disharmony in the young child is a Retrognathic maxilla with normal mandibular length. These cases are more frequently seen in younger children with extensive airway problems. 7, 8, 9 The molars exhibit a Class III molar relationship between ½ to a full cusp mesially (4-6mm). Usually there is both posterior and anterior cross-bites with a reverse incisor relationship. The incisors may exhibit either a deep bite or open bite depending on the lower mandibular plane angle. The “wits” appraisal ranges from -2.0mm to -7.0mm. The lower mandibular plane angle may be either less than 20.0 degrees (skeletal closed bite, hypo-divergent) or greater than 30.0 degrees (skeletal open bite, hyper-divergent). Often, there is mid-facial deficiency. The faces of the patients are usually brachy-cephalic in closed bite cases and dolichocephalic in open bite cases. Treatment is principally directed, following ENT evaluation, at the retruded maxilla and cross-bites. Treatment should be initiated before the age of 10 years according to most studies published. Banded rapid palatal expander (RPE) may be employed in the deep bite cases while a bonded occlusal coverage RPE should be utilized in the open bite cases. This is followed by 8-9 months of a Reverse Pull Face Mask (RPFM). A regulator or Frankel-III may be used as a removable reten-tion appliance until Comprehensive Orthodontics is initiated. Alterna-tively, a palatal bar or Molar Rotator (MR) may be placed on the upper first molars after face mask therapy for anchorage followed by UAW’s and then Comprehensive Orthodontics with a pre-programmed fixed appliance. It is not uncommon for this type of Class III patient to undergo three phases of treatment. A stable, fair to good prognosis would be predicted. However, cases should be moni-tored until the age of 18 years old especially for the male patient with a familial history of Class III. (Fig. 3) The use of serial cephalometric radiographs taken a few years after Face Mask treatment and a Growth Treatment Response Vector (GTRV) using the Wits analysis to individu-alize and enhance the accuracy in predicting excessive mandibular growth has been proposed. 10, 11 Type 4 Prognathic Mandible Class III The Type 3 could harbor Type 4 with expression of latent excessive mandibular growth. This genetic problem is difficult to treat and fore-cast in the young child with mixed results predicted non-surgical. Continued care with either inter-mittent face mask therapy or chin cup therapy may be indicated depending on the severity of the prognathic mandible. Treatment must be initiated before the age of 10 years for maximum growth modification and to be in the range of camouflage definitive treatment if needed. Parents should be informed of potential orthognathic surgery at a later date if treatment objectives are Fig. 3 RPE RPFM www.orthodontics.com March/April 2013 27
Journal of the American Orthodontic Society March-April 2013: Page 27